

Australian Deaths reported following Vaccination
Comparison with COVID Deaths

Deaths caused by the mRNA vaccines have come into focus since the release of the first large tranche of 10,000 pages of the Pfizer documents, following the successful court order to release them in the United States.
Here I compare the deaths due to COVID with deaths reported caused by vaccination in Australia.

In Dr John Campbell’s video from 9th of March, he looks into the first release of Pfizer data. Originally the FDA and Pfizer tried to delay the release of this data by 75 years, so that anyone vaccinated with these vaccines would no longer be alive to see the full release!
Dr Campbell’s videos have been a calm, trusted source of information throughout the pandemic. Typically, there are up to 1M views per each roughly 20 min episode. This one currently has 2M views. He notes that from this data in the first 3 months from release of the vaccine (Dec 2020 – Feb 2021) there were:
42,000 adverse events
1,223 deaths
At the 5 minute mark he notes: “It would have been good to know about this at the time wouldn’t it?” At the 6 minute mark he refers to a redacted piece of information which is the number of vaccinations delivered. “Why would they want to redact that information? … Why wouldn’t we be able to access those percentages?” He is beginning to look angry.
In Australia we have sub standard reporting systems but we can try our best to assess what is going on with respect to deaths cause by vaccination.
I became aware of a Therapeutic Goods Administration (TGA) Freedom of Information (FOI) request from another substack article. In that post there is a reference to the work of a German analyst who looked at this data. The FOI document is highly redacted, making it very confusing. Apparently the FOI request asked for the ages of all deaths reported due to vaccination, so that’s all you get.
The first 28 pages of the document contains a list of ages in an unredacted column of what appears to be a table. I copy pasted these from the pdf into a spreadsheet to start working with it. There are 921 values, 33 of which are null values (presumably where age was not recorded properly).
I suspect the order is chronological order of occurrence as there appears to be a trend from older ages to younger. The document has a total of 192 pages. Some people looking at this document have assumed there are similar records per each line on the remaining pages and this assumption leads to over 6000 reported deaths. I will stick with the explicitly listed ages in this analysis (921 deaths from March 2021 to January 2022).
The annoying thing is that under a FOI request, there was no attempt to stop all this confusion. Blacking out everything except the list of numbers and leaving hundreds of pages blacked out is ridiculous. Surely it would have been simpler to provide a curated data set to avoid confusion. Just like the redacted number of vaccinations in the Pfizer documents, clearly this is obfuscation to hide numbers that are not showing desired results.
However, having a full set of ages is useful. Stratifying against age is crucial for all analysis related to COVID. I want to compare these deaths from vaccination against the number of deaths due to COVID.
In a previous substack article I have referred to a release of information from the Australian Bureau of Statistics (ABS). This provides an age stratification of all COVID deaths in Australia. A limitation is the banding of younger ages 0-39, presumably due to the small count over that range. Otherwise age bands are 10 years. Also all ages greater than 90 are banded as 90+. The raw numbers from this graph are able to be downloaded and we can add male and female numbers to get a total.

Now these numbers are from the start of the pandemic to the date of release (ie from March 2020 to Jan 2022). To get an estimate of COVID deaths against age over the period of vaccination I have to make an estimate. Looking at COVID deaths by month in Australia:

we can calculate the fraction of deaths over the vaccination period (Mar 2021 – Jan 2022) compared to total pandemic deaths (from Mar 2020) and apply this factor to the COVID deaths vs ages data. The fraction is 0.64. Of course, this makes an assumption the effect of death vs age remains constant over time. There may be changes to this relationship due to virus variants.
So now we plot, for the period of vaccination in Australia, the adjusted COVID deaths vs deaths reported due to vaccination, against age bands.
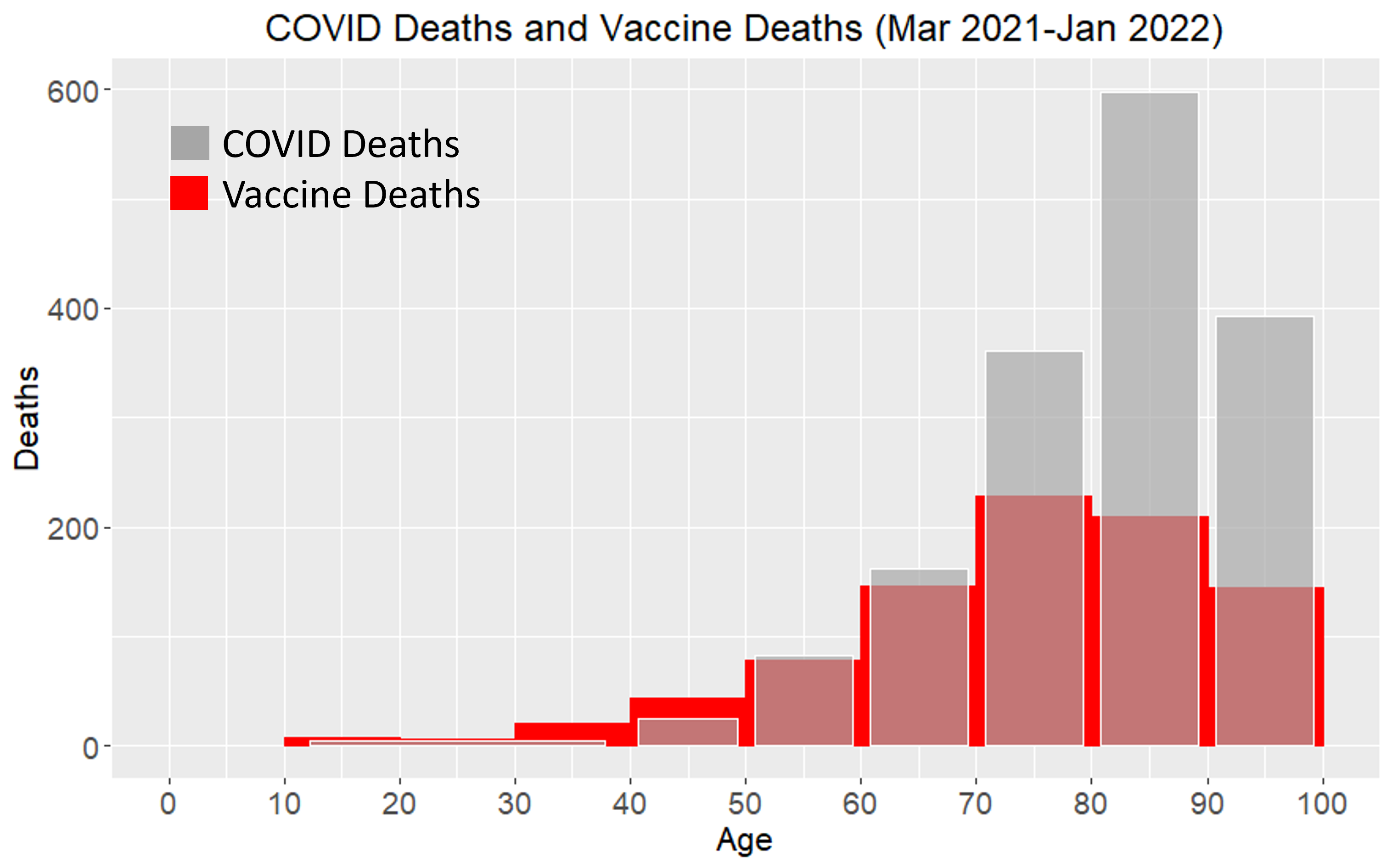
COVID Deaths, estimated per age band, are the grey (transparent) bars. For the 0-39 age band I have spread the deaths evenly over the 10-39 age band. Total COVID deaths for ages under 40 is small (25 for whole pandemic so far, smaller when adjusted for the date range).
The impact of COVID for ages over 70 is significant. However, so too is the reported deaths following vaccination, ie the red bars in the graph. Unfortunately, health agencies try to hand wave this away as they say people die anyway so you can’t say it is due to the vaccine. The number of deaths that the TGA positively attribute to vaccine is miniscule compared to the reported deaths. It seems obvious if there is a report made there is likely a causal effect.
When someone is in their 100th year and they die shortly after vaccination it will naturally be difficult to establish a causal effect. However, if there are significant number of deaths due to vaccination in the age group this leads to an ethical question of why don’t you leave them alone?
The data I would want to see is the date of last vaccination and date of death for each individual. Even if medically it is difficult to attribute the cause, particularly in the presence of comorbidities, we can statistically estimate the likelihood that death was caused by the intervention. For example if the majority of deaths were within a certain number of days of vaccination then this would be very suspicious. The unfortunate thing is we may never see this data.
At younger ages the probability of dying within a certain number of days from some intervention is obviously lower than it is for the elderly and frail.
Alarming
When we look at the numbers for working age people, ie <60, the result is alarming.
There are more suspected deaths from vaccination than there are from COVID!
A death, suspected as being from vaccination, in this age group is unlikely to be from some other random cause.
There is now a moral question of whether you can force someone to take a treatment for a disease when there is more chance that they will die from the treatment than the disease. I wonder whether in the history of medicine there has ever been such a situation forced upon people? An argument could be made “oh but many more would have died without the treatment so it is acceptable”. But lives saved by vaccination doesn’t stack up based on current data. In any case I would imagine that the ratio of people you are prepared to sacrifice to the number saved should be very high, like thousands of times.
We also know that the current vaccines do not stop infection as promised but rather they amplify infection rates in the vaccinated (from other analysis on UK and NSW data). For those under 60 we have a treatment that is more likely to cause death, than the risk they have of death from the disease itself.
There is currently a call in Australia to “immediately halt the use of gene-based vaccines to the Australian public”. This is in an open letter written by the COVID Medical Network. This is an association of doctors, lawyers and academics. The letter is addressed to the organisation responsible for approving vaccines, the Australian Advisory Group on Immunisation (ATAGI), Department of Health bureaucrats and the Health Minister. This document is a very good summary and worth looking at. It is detailed (52 pages) and provides all references. It goes into alarming figures of increases in all-cause mortality around the world. The graph for Israeli all-cause mortality for over 85’s (p27) is terrifying. Peaks occur at each of the 2nd shot and 3rd and 4th booster shots (and the trace for the 4th hasn’t finished yet).
The document notes under-reporting in the Adverse Event database in Australia (p18). Another interesting reference is the German post vaccination autopsy findings. A causal relationship was found for 30-40% of all suspected deaths. This is applied together with an under-reporting factor and an estimate of deaths from COVID-19 vaccination is between 2275 and 6501. So it is quite possible that the deaths from vaccination, the red bars, are higher than I have shown in the graph. COVID deaths on the other hand are not likely to be underestimated. Many will have been deaths with COVID, rather than from COVID.
On ethical grounds there is no justification to mandate a vaccine that is more likely to cause death in people of working age. Together with the increased rate of infection in the vaccinated in the presence of variants, this is shaping up to be one of the biggest scientific and bureaucratic blunders in human history.