Australian Excess Mortality - continued

Excess Mortality is a topic in focus. This article follows on from my previous one. I’m learning how to improve my descriptions of data when there is only limited space. Thanks for all the feedback. I’ve also realised I have to be smarter with my use of colour scales when there are many in the population with different types of colour blindness.
In my last post I showed Excess Mortality in Australia based on a recent release of data from the Australian Bureau of Statistics (ABS). I showed data for the last two years (Jan 2020 to Jan 2022). There are some concerning trends emerging as 2021 progresses. However, I realised that looking at the last two years alone doesn’t allow us to see the trend that is occurring. So, I have calculated the Excess Mortality from 2015 onwards and plotted it. The years pre-pandemic 2015-2019, used to calculate a baseline, are what we consider “normal” and the excess is compared to that.
So Excess mortality during “typical” years looks like the following:
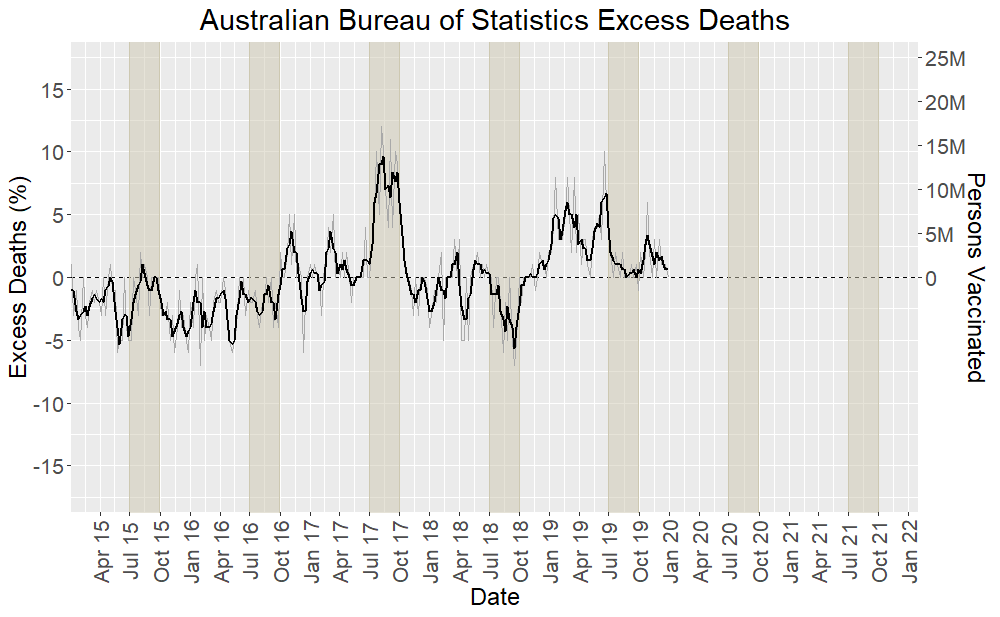
The Excess Mortality hovers around zero. The typical maximum deviation from zero is ± 5%. However, we know the Winter of 2017 was a bad influenza season. We can see a peak in Excess Deaths in that winter, almost reaching 10% excess. Winter in the Southern Hemisphere is June-August. The flu season is generally shifted by one month and I have highlighted the months July to September (ie Quarter 3). I show the actual week to week numbers in light grey and the black line is a 3- point average to smooth it out.
For reference, below I plot the actual number of deaths in Australia for years 2015-2021 and the calculated baseline.

Two baselines are shown, one for a mean and one for a median calculation. They are the thick dashed lines in brown and red respectively. I have used the median for the baseline in my Excess calculations as that handles unusual outliers better. You can see they are similar with the mean baseline slightly higher in the Winter months, driven by the abnormally bad flu season in 2017. The deaths for each year are in the thinner lines with different years shown in colour in the legend. The year 2017 is the light blue line and 2021 is the orange line. It is clear 2021 is very different to the baseline.
Now we extend the first plot shown in this article with the Excess Mortality for pandemic years 2020 and 2021.
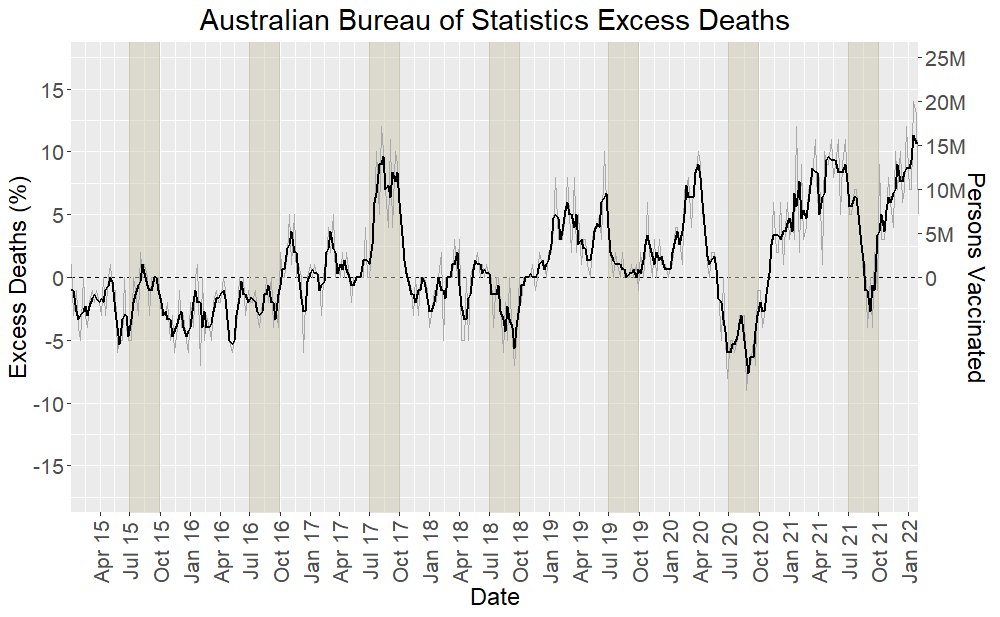
The divergence from the typical trend is clear. Note that all COVID deaths have been subtracted first. So the excess does NOT include any COVID deaths. Values above zero are therefore unexplained deaths. Anything above 5% is unusual. In the plot below I have annotated the plot with various features of interest.

Australia implemented a COVID Zero policy and a hard lockdown until the end of 2021. There was minimal influenza for both Australian Winters of 2020 and 2021. Because the baseline being subtracted is high during these periods, due to typical influenza season, this puts two dips in the Excess Deaths plot. So, we look for a trend ignoring these dips. The excess deaths outside Winter show clearly higher than normal Excess Mortality. There is also a peak early 2020 when the lockdowns commenced. Also shown is the vaccination rollout starting in March 2021. Number of persons with first jab is shown in a blue line with axis scale labels on right hand side.
What are the possible cause of excess deaths? They include:
Consequences of lockdowns, eg suicides, drug overdose, elderly dying in despair or from lack of care.
People not attending medical appointments and missing early diagnosis.
Collateral damage from vaccination rollout. We know there are acute adverse events and death resulting from administration of COVID-19 vaccines. We know from worldwide reports that the non-compulsory reporting systems are highly underreported.
Long term effects of vaccination slowly being uncovered.
In the graph below I have plotted the number of persons vaccinated since the start of vaccination in Australia and the number of reported deaths from vaccination. To be clear the vertical scales for each line are not the same. Total persons vaccinated (at least one shot) in Australia is approximately 20M. Number of reported deaths from vaccination is approximately 800 (Mar 2021-Jan 2022). Under-reporting factors of up to 30 have been suggested for the US VAERS system. 800 deaths over a year is approximately 16 deaths per week. Using a scale factor of 10 would mean 160 deaths. An average number of deaths per week in Australia is 3100. An increase in Excess Mortality of 5% would result from 155 additional deaths per week.
They are plotted together to show the relative rates of increase. The elderly were the first to get vaccinated and we see a higher rate of reported vaccination deaths early on in the rollout. This is consistent with the age spread of deaths from vaccination we have looked at in a previous newsletter.
The Australian legacy media has acknowledged the increase in mortality but are unable to acknowledge failures of Public Health measures and appear to be deflecting to indicate people are not taking COVID seriously. An article from the Age newspaper states: “We’re living with COVID but more of us are dying than ever. Once a daily obsession, Australians now seem largely inured to the sobering daily stats from the ongoing pandemic…”
An “expert” in the article says “low childhood vaccination and third-shot booster rates, along with the relaxation of mask and isolation restrictions while still in the peak of the Omicron wave, were leading to increased transmission”
This is completely useless information. More and more studies are showing the ineffectiveness of masks and lockdown restrictions now we have some longer term data.
More and more real-world data is coming out showing that infection rates in the vaccinated and boosted is increased over the unvaccinated. It has been seen for some time clearly in UK and Australian data (which I reported in my early newsletters). For Denmark, see a recent substack article from Joel Smalley: “Denmark pandemic of the Vaccinated”.
Recently the US pharmacy, Walgreens, has published their own data and this has been reported on by Jefferey Jaxen. You can find the Walgreens tracker here. This is the most recent update as I took the screen shot it, so slightly different from as shown the Jaxen report.

There’s not room to go into it here but Geert Vanden Bocsche has made dire predictions regarding the mass vaccination campaign in his final call to the WHO.

He’s been right about everything so far.
In The Guardian article from 7 May 2022: “Explainer: why are Covid infection rates in Australia so high compared with other countries?” In this article another epidemiology expert in Australia (who has been quiet for a while) states: “Australia’s high reported infection rate may be the result of high case ascertainment”. High “case ascertainment”, well there’s a new term for the pandemic. In Australia we try to say we are too good at finding infections. In other countries where infection and death rates are lower they must not be counting it properly, eg India.
This speculation on high case ascertainment is based on trying to compare ratio of deaths rates and infection rates in UK and Australia, which you would expect would be similar, all other things being equal. This is all confounded of course by more tests meaning more false positives.
Irrespective of whether vaccine is protective, more infections means more deaths.
We have also learnt recently that the week after boosting there is an increased risk of infection due to suppression of the immune system as the vaccine does it’s thing.
Australia and New Zealand currently leading the World
Australia currently has the world’s second highest infection rate behind only New Zealand. Both countries having attempted COVID zero policies which failed and have amongst the world’s highest vaccination rates.
The Age newspaper article refers to the ABS Excess Mortality data showing a 22% increase in mortality in January. However, it implies the excess mortality being seen is all due to COVID: “The COVID-19 deaths – those doctor certified and coroner referred, meaning there could be more to be reported – led to a 22.1 per cent increase in overall deaths compared with the January average.”
However, this is misleading. In January 2022 the increased Omicron deaths in Australia are only starting, In the plots above COVID deaths have been subtracted prior to calculating Excess Mortality.
For reference: in 2020 there were 909 deaths. In 2021: 1313 deaths and in 2022, till 7 May, the article reports there have been 5269 COVID Deaths. The majority of deaths in Australia are after January 2022.
To finish off I saw a recent episode of the podcast UnHerd with guest Danish Professor Christine Stabell-Benn.

Her group studies the effects of vaccines on excess mortality. This is something that they routinely study for all types of vaccines. It was interesting to hear this because the mainstream narrative seems to want to know nothing about excess mortality. Apparently, it is well known that while some vaccines reduce the disease they are targeted at they also cause other problems leading to a reduction in the overall mortality benefit. Some vaccines have worked against a disease and beneficially reduced other disease as well, leading to further reduced mortality.
They compared adenovirus-based vaccines (AstraZeneca) and mRNA vaccines (Pfizer, Moderna). They had limited data but the result of the study is that adenovirus vaccines showed an improvement in overall mortality. mRNA vaccines showed no difference in mortality compared to unvaccinated.
What this means that if the mRNA vaccines are so good at reducing deaths due to COVID-19 they are doing something else that leads to deaths such that there is no overall mortality benefit. This shouldn’t be surprising because in the Pfizer trials more people actually died in the vaccination arm of the trial compared to the control unvaccinated arm of the trial, irrespective of COVID-19.
When pushed by the host Freddy Sayers to say something controversial she couldn’t justify vaccination with mRNA vaccines for anyone over the age of 50.
Again, the Danish seem to be good at plainly speaking as I discussed in an earlier newsletter on modelling.
That’s all for now. Stay safe and effective…
Hi Andrew
Just curious. Did you do a regression of of the excess mortality line?
It looks like it would have a positive slope i.e. General mortality trend looks to be on the rise. Not sure why? In general I thought the consensus was that we were supposed to be getting “healthier” over time. It’s possibly due to the aging population or the decrease in health funding to the stars by our current federal government or maybe something completely unrelated.
I realize you’d want (need) it flat because your using it as “the baseline” and your intent is to get a baseline to compare 2020-2022 to 2015-2019 and your goal was not to compare mortality in general over time but to compare the periods in question. I’m just curious and interested in knowing if the trend was already on the way up before the pandemic years?
Thanks…..
Hi Andrew
Thanks for another absolutely awesome article. You’ve really outdone yourself with this one.
I hope your reference to colour blindness wasn’t a little dig at me 😎. It wasn’t the colour that was an issue it was more me not wearing my reading glasses 🤓and probably some “selective vision”. I wasn’t expecting the big spike at the end in January, so I didn’t see it. A bit like the selective vision of our media and government. The vaccines are supposed to be safe and effective any evidence to the contrary is not welcome in their minds, so they don’t see it. It’s just not what they’re expecting.
……….. Begin Rant ………….
I’m surprised (not really) that this is not being investigated by academics who can get access to more granular data. I mean this with no disrespect, but you are a private citizen looking at the limited publicly available data and your doing an excellent job. I’m pretty sure there is more undisclosed data behind the scenes that we are just unaware of. It shouldn’t be left to people like you (or me) to do this sort of work. Our tax dollars are actually paying for “real statisticians”, “real epidemiologists” and “real scientists” to do this work, instead it looks like their time is being spent putting out advertisements for the pharmaceutical companies and telling us “How good is the vaccine 👍!”. They should get off their asses and look into it.
……….end rant……..
Thanks…