Could Vaccination be more Effective against COVID Infection "Down Under"?
Simple answer: NO

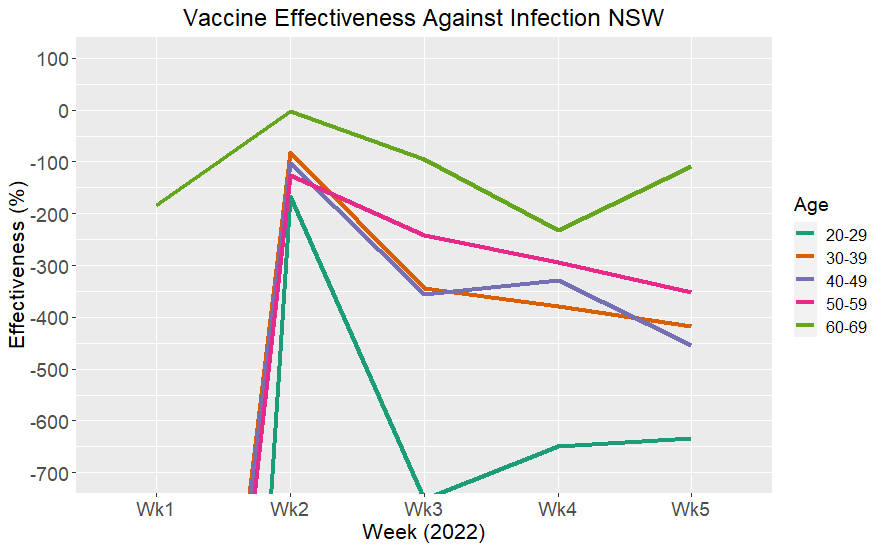
The bar chart below shows Vaccine Effectiveness for the latest weekly report from the state of New South Wales (NSW) in Australia:

I was showing this to someone not paying particular attention to the impact of the pandemic. They commented “isn’t this graph upside down?”
Understanding this real world data is important. In Australia the Federal Government abdicated its role in mandating vaccination. It was left to individual institutions, following state health bureaucrat expert advice, as well as based on participant surveys in the midst of fears generated, that the unvaccinated posed a risk to society. Decisions have been made by companies and institutions to mandate vaccination. Otherwise lose your job. Some organisations are still even mandating boosters for those who have already had two shots plus recent infection with Omicron.
Therefore, the basis for these decisions needs to based on real world data, not promised product data. Also, there are potential long term health effects, if the natural human immune system is being compromised by the intervention.
There were challenges in extracting the data required. I will dive into the details of this later. I have structured this article so those who want to go into the details can do so in the later part of the post.
The top line results are here. Effectiveness is meant to be positive. When it is negative it means that the treatment is making things worse. Another way to understand the data above is to look at the raw case rates:

This graph shows the rate (per week) of infections on the vertical axis with unvaccinated cases shown in blue and vaccinated cases shown in orange. These rates take into account the different proportions of the population for each vaccination status. It is clear that vaccination does nothing to reduce chance of infection with Omicron.
In fact, it makes it worse.
Looking at how Effectiveness changed over the period for which I could calculate it:

Effectiveness went through the floor in Week 1 of 2022. I clipped the scale on the Y axis intentionally, as values for Week 1 are below -1000%. This reporting week (ending Jan 8) covers our Christmas, New Year holiday period. Those infections would have come from contacts the week before and during the week of Christmas. In Australia it is Summer and traditionally the time for work Christmas parties and family get-togethers. After the 15th December 2021 in NSW many of the harsh restrictions were lifted and the unvaccinated could go to restaurants and shops, etc. Vaccinated people may have thought they had a magic shield, but like the Emperor’s new clothes there was nothing there. So, data for this particular week may be biased. Vaccinated numbers could also be inflated by people getting tested in droves that week, required in order to travel interstate, and the false positives from PCR testing affecting the result. The PCR testing regime broke down this week.
In my first substack post I looked at UK data on infection rates from surveillance reports. It’s taken some time to get my head around the Australian reports. We have to look state by state in Australia to find data as there is a very poorly coordinated federal response. I report here on data from New South Wales (NSW), the most populous state in Australia, currently in the midst of Omicron infection (hopefully the tail end). In Australia different lockdown rules mean the pandemic is playing out differently. One state, Western Australia, is still locked down but facing the prospect of thousands of cases per day on the population naïve to any infection for over 2 years.
The NSW data above is consistent with that from other countries. A comparison with UK data I used previously shows a very similar trend:

I understand the same thing has been seen in Denmark, Canada and other countries. The real-world data is implying that there is an infection enhancement effect.
I don’t want to make too specific comments on the possible causes, even though like many people, we have learnt more in the last two years about immunity and vaccinology than in all our previous life. I want to keep my newsletter strictly on the data. All I can say is that everything that has been said by Geert Vanden Bossche makes sense in the light of this data. It has been predicted by vaccinologists that vaccinating with the wrong type of vaccine can suppress the innate immune system.
People have lost jobs due to vaccination mandates, stemming from the erroneous belief that they pose a health risk in the workplace. The data from NSW shows if anything it is the other way around. The innate immunity of the unvaccinated needs to be preserved.
The unvaccinated pose no increased risk to workplace health and safety.
For those who want further insight about how these numbers came about read on…
Method
The surveillance reports are confusing. Besides reporting, they try to drive the narrative, as I found in the UK reports. I believe the narrative should be separated from data in the reports. Data is often unhelpfully aggregated. There are examples where totals for unvaccinated include cases for age groups where vaccination is not approved. When numbers go beyond certain values resolution is lost eg values like >95%, <1% are reported. Figures you need are sometimes only provided in a graphic. However, with patience it is possible to draw out relevant numbers, and taking into account known uncertainties, we can make reasonable estimates.
So, we start with the NSW weekly surveillance reports. The focus in the report is on aggregated data although the Surveillance Report does give a weekly number of deaths compared to the previous week. A table from the Week 4, 2022 report:

This table gives us the numbers of infection cases for 10-year age bands against vaccination status. This information has not always been provided. It appeared in the reports in Week 52 in 2021 (the week ending 1 Jan 2022). The reports also appear to be released to the public for data about 3 weeks behind current time. So, a decision to change reporting structure is probably based on data known several weeks in advance.
The intention of the table, as described in the text of the surveillance report, is to show that the ratios of “severe outcome” (defined as ICU or death) to number of infection cases, is smaller for the vaccinated versus unvaccinated. I will deal with this in another post. The numbers are cumulative from 26 November 2021, which was approximately the start of the Omicron variant infection in Australia.
We can look at the cumulative numbers but, as I found with the UK data, it is useful to track how things change with time. From weeks 52 to Week 5 (most recent at time of writing) we can get weekly numbers by subtraction of the accumulated numbers (for weeks 1 to 5).
Here we are interested in the rate of infection between groups with different vaccination status for different ages. This is a crucial measure. The implication has been made by health authorities and “experts” that the unvaccinated are the cause of infections. We have seen from data in other countries that this is not the case. We want to know what it is for New South Wales.
To give an idea of daily cases in Australia compared to UK and a few other countries see the graph below from the Our World in Data site for the period of interest (Nov 25, 2021 to the day I captured it on 19 Feb 2022). I add Africa and Israel for reference.

Note the Y axis is in daily cases per million and a 7-day average.
Of course, conclusions should not be drawn from the relationship between overall rate of vaccination in the county to the peak number of cases in the countries shown.
In Australia, at the peak in early January, daily cases per million are approximately 4000. Converting to per week and per 100,000 this gives a case rate of approximately 2800. The UK peak is a bit over half of that value.
A thing different about the situation in Australia, compared to many other countries, is the hard international border plus severe restrictions over the last two years. We have gone through two winters with almost no cases of seasonal flu. There were a relatively low number of cases of COVID preceding the onset of Omicron. So, the majority of people would not have any natural immunity from previous infection. In my report on UK data, I found the UK reports suggested that unvaccinated case numbers were influenced by fact that they may have had previous infection therefore reducing those numbers. So this will not be the case in Australia. See the graph below, which starts from beginning of the pandemic. There are relatively low number of cases in Australia preceding Omicron compared to other countries. India is shown this time for reference.

Severe Outcomes
A brief comment on this before I go back to infections. Going back to the table from the NSW Surveillance Report. I note that the number of severe outcomes is small, of the order of 10’s, for both groups less than 2 effective dose and 3 dose. If there is a small number amongst them, due to some other effect, this is where a bias can have a big effect. I will address these numbers in another post. We know that those most likely to have severe outcomes unfortunately have bad health, with severe comorbidities. The ABS statistics from my previous post:
show that COVID deaths comprise over 90% with severe comorbidities. However, we are also told that the main proportion of severe outcomes are those who are unvaccinated.
Why have these people not had vaccination?
There are certainly medical conditions where vaccination not recommended by the individual doctor. Government information says this is rare. Patients maybe near to end of life. We know that the age of death from COVID is the same at the life expectancy for both males and females.
No studies of this effect have been done. This is either incompetence or intentional.
There have been doctors calling out to charge full cost to those unvaccinated in hospital with COVID, filling up the ICU. So, a dementia patient near end of life that had not had vaccination should be charged out of pocket? It beggars belief that health professionals have said such things.
Another fundamental problem with the NSW data is the combining of those who had one dose with no dose. This is based on the definition that those who have not had the two shots are not “fully vaccinated”.
Those with one shot, now we are well into the pandemic, are clearly a distinct group and need to be separated out in any analysis. This has been shown in Professor Fenton’s work and others.
The primary reason people have only one dose can only be because they have had an adverse reaction to the initial vaccination. It is hard to find any other reason, particularly in countries with severe mandates such as Australia. The draconian measures in Australia mean that anyone who has chosen to have the initial dose, and not had an adverse effect, will go on to have the second. Otherwise, they will lose their job and not be able to do other activities. It won’t be because they are lazy. Politicians were always boasting based on the first jab percentages that everyone who gets the first will go on and get the next. But there is a stubborn percent in each age group that have only one dose.
If people have an adverse reaction to the first jab, reasons could include because of pre-existing health conditions. It could be a specific reaction to the spike protein generated by the vaccine itself. If so, one presumes they will also react badly to COVID itself.
We want to get an estimate of the rate of infection for different vaccination status. This turned out to be difficult because of the muddled way reporting is done in Australia and in the states. The problems with the way reporting is done would take a volume to write up but I will highlight a few of the things I came across.
Populations could be found for each of the age groups in NSW based on a 2020 census (in 5-year age bands). I cross checked these numbers with others inferred in the report to be confident they are consistent. This is important so I am using approximately the correct denominator for the rate calculation. However, if this is out there will be the same relative error in each vaccination group.
We need to know the percentage of population in each vaccination status within each age band. As far as I could tell this information is not made available directly. There are graphs provided on some web pages. See for example for 22 Feb, 2022:

This is another challenge with the data. Sometimes data is provided on web pages and updated daily, so unless you recorded it each day, history is not available.
If you roll the mouse over the interactive bars on some graphs on web pages you can see numbers. For example, for the 30-39 age group, 2 dose and one dose, are 93% and 94.9% respectively (ie almost 2% with one dose only and 5% unvaccinated). Above 95% the graph only shows >95% so you can’t read off it directly.
So long as there are a few percent of unvaccinated we can still make valid estimates. The population of the 30-39 age group is approximately 120,000. 5% is 6000 people.
For ages above 60 it was difficult to make accurate estimates. So I will focus on the 4 age groups between 20 to 60 years.
It is assumed that the fully vaccinated in the graph above includes 2 or 3 doses. For Australia, overall 3 dose coverage is approximately 50%. But the 3-dose coverage for the state and age bands is not provided. So, I assume we are combining 2 and 3 dose.
Vaccine information is rolled out on a daily basis and it is mainly about cumulative number of jabs rather than providing useful breakdowns. You can find a daily rollout update. They are sets of slides updated each day. The only dataset available covers the whole of Australia and has no state, age and status breakdowns. However, there is a jurisdictional slide pack that contains a state graph that we can use.

The horizontal bar chart indirectly has the data we need. Data is shown separately for male and female and so we can add these. Percentages are shown in a table on the right of the slide for 5-year age bands, so we could average these to get a 10-year age band but unfortunately above 95% they didn’t see the need to show the actual number. Also strictly averaging the rates is not correct. The way I decided to do it was to read off the graph the actual numbers of persons according to the scale. To make reading off the graph as accurate as possible I did a screen shot, zoomed it up, and used the cursor in image editor software to read off the nearest pixel for each of the bars. I found I could pick the nearest pixel. When comparing the population values I found I could estimate to within +/-500 of population from Census data. So that gave me confidence in the method. Then combine data for the 5-year age bands. Add male and female. The percentages I calculated agreed to within 0.5% of numbers in the table above for 5-year age bands (where it was less than 95%).
There is no indication of 3 dose. It is assumed fully vaccinated means 2 or 3 doses.
I also took the graphs from reports for the start of the period of the data in the table to compare and worked out the same percentages. They moved less than a percent over the period. I therefore took percentages at the end of the period for working out rates as this would underestimate any benefits of not being vaccinated, ie so the unvaccinated group is at its smallest.
So, using the percentages for each vaccination status and the populations for the age group, combine this with the number of cases provided in the surveillance reports, we can calculate Vaccine Effectiveness in the population.
We have the cumulative values over the period 26 Nov 2021 to 5 Feb 2022 and we can work out weekly values for Weeks 1 to 5. The following graph was shown earlier in the article:
Case Rates
For comparison of actual case rates I produced the same 3D bar graph, as shown at the beginning of the article, for the UK data I analysed previously (also shown in first section). I note that I had to check that my rates were consistent. The UK data reports over a 4 week period. For example for Week 2 report it says it is for between week 50 and week 1. I realised I wasn’t sure what “between” meant, ie is it inclusive of the end weeks? I checked various other rates to be convinced it is in fact the 4 week period. I adjusted values so that they show a rate for one week, as I have calculated for NSW data. This is another annoyance with analysing these reports, ie the vagueness of definitions.
Looking at the graph for case rates for the UK shows a similar structure to what is found for the NSW data.
Infection rate is higher in all age bands for the vaccinated. There appears to be an increase in this trend for younger age groups.
Also, I have been reading the NSW Surveillance Reports for a while now and have noticed the subtle shifting in the way the tables and comments are reported to make “excuses” for declining vaccine effectiveness. Have a look at the “cleansing” that took place between Delta & Omicron, this report was very slow to be released publicly. Maybe they were short staffed, it was released by NSW Health close to Christmas during the school holidays, so they may have had staff on leave or isolating due to Omicron. Note: the report date is not the date they upload it to their web site.
Hi Andrew, great analysis. Your analysis and methods are pretty much in line with what I’ve found. The “negative” effectiveness has me baffled, being negative would imply the vaccinated are more susceptible to Omicron than the unvaccinated, this I find hard to believe. I think if you use the same technique you’ll probably find the effectiveness is overstated for the vaccinated in previous periods due to issues in the denominator “moving” in time. If you look at the U.K data video posted by Gaz in another thread you can see it go from +ve to -ve then moves back up towards 0, my guess is both 2 and 3 dose will go positive again as booster dose “kicks in”. Why would the number of boosters effect the 2 dose effectiveness? It doesn’t make sense. My conjecture is that it makes sense if you don’t properly account for people entering and leaving the group over time. I think Dr Fenton refers to a “so called deadly first dose” in one of his videos and uses an analogy where he refers to it as something like moving from a fox hole to a safe bunker and having to cross a mine field to get to the bunker and misclassifying the mine field deaths as foxhole deaths or something like that. I think it's the video where he discusses the paper below: https://www.researchgate.net/publication/356756711_Latest_statistics_on_England_mortality_data_suggest_systematic_mis-categorisation_of_vaccine_status_and_uncertain_effectiveness_of_Covid-19_vaccination
I think he’s onto something, he suggests the effects are due to misclassifications more than anything else. The “under investigation” in NSW data could also be a clue.