
Don’t ask Questions that you don’t want the Answer to
Don’t ask Questions that you don’t want the Answer to
Thai Children Myocarditis Study

The COVID news in the recent week is dominated by a study from Thailand on myocarditis in teenagers, following injection with Pfizer BNT162b2. In this article I take a look at the myocarditis seen in the Australian TGA adverse events database.
I find it intriguing, when you try to make no assumptions about what you will see and after you find the data and run some code to display the property you are interested in you get what has been found in other countries. It is a curious experience.
There is plenty of commentary on the Thai study. This interview by Kim Iversen with Dr Peter McCullough, who is a cardiologist, is good.
He calls it as it is. “How come Harvard didn’t do this study? how come Mayo Clinic didn’t do it? …”
Cardiovascular effects were found in 30% of the children, ranging from racing heart rate (tachycardia) to inflammation of the heart (myopericarditis), 7 of the 301 teenagers (ie 2.3%) in the study had a serious heart problem, 3 had either myopericarditis or pericarditis and also had pericardial effusion, which is fluid around the heart. Four had subclinical myocarditis (explained below). One was admitted to Intensive Care Unit (ICU).
It is noted that all children recovered after treatment, but as Dr McCullough notes there is no case of mild heart damage.
Dr McCullough at 5 min 30sec in the interview:
“…the implications are unknown but I can tell you as a cardiologist, heart damage causes scarring, and where there is a scar that’s a setup for an abnormal heart rhythm and that abnormal heart rhythm can lead to a cardiac arrest …. when there is superimposed adrenaline or noradrenaline as in exercise it is the trigger for cardiac arrest and it may explain why we have seen scores of athletes die on the field or die during training or other event because it is subclinical myocarditis and then superimposed adrenaline surge.”
The important points from this study are the higher incidence of heart problems, than seen in other studies or surveillance. They also looked for what is called “subclinical” heart problems. That is where there is no external manifestation of the problem (like chest pain) but some damage has been done. They find this by measuring certain chemicals, one of which is a protein called Troponin. Troponin is normally in heart cells and works as part of the contracting function. When heart cells are damaged it is released and goes into the blood stream where it can be measured.
Other commentary is by Dr John Campbell:
and Professor Vinay Prasad:
This appears to be the first such “prospective study” since the rollout of injections. From this stats webpage: a prospective study watches for outcomes, such as the development of a disease, during the study period and relates this to other factors such as suspected risk or protection factor(s).
Both commentators have a sense of indignation. Why weren’t these studies done in the US or UK? Really, I think most awake people know why.
You don’t ask questions for which you don’t want the answer to.
This Thai study is well executed and written, but I would assert it should not be that difficult a study to perform. It could be run in any country with the desire to understand risks to the health of their population. The hard bit would be organising all the permissions. The schools that the Thai doctors worked with are to be commended.
Modern cardiac monitors have the function to assess heart rhythms. You get a blood test before and after and tick a box on a form to specify measure Troponin-T level, and enzyme CP-MB (Creatinine phosphokinase (CP) and myoglobin (MB)). At the end you count how many had adverse outcome, based on the heart rhythms and the enzyme levels.
The major health agencies apparently can’t do it.
From legacy media (Disney owned ABC) December 2021:
With nearly 5 million children getting COVID vaccines, no safety problems have been seen, CDC director says.
Really? It goes on:
“With nearly 5 million children ages 5 to 11 now vaccinated against COVID-19, Centers for Disease Control and Prevention Director Dr. Rochelle Walensky says real-world monitoring finds vaccines are safe for young children.
Crucially, the CDC hasn't identified any concerns with the temporary heart inflammation known as myocarditis, a potential side effect of mRNA vaccines seen in rare circumstances in teenagers and young adults.
"We haven't seen anything yet," Walensky told ABC News Chief Medical Correspondent Dr. Jennifer Ashton in a rare in-person interview from CDC headquarters in Atlanta. "We have an incredibly robust vaccine safety system, and so if [problems] were there, we would find it."
Walensky (woman in a blue jacket), seen above, must know there are no safety problems because she is monitoring some big screens with colourful charts in the CDC headquarters. But look maybe she’s spotted something!
Unfortunately though, they couldn’t do any studies of a few hundred children.
Australian Analysis
Since June 2022 the Australian Therapeutic Goods Association (TGA) has a “beta” version of the Database of Adverse Event Notifications (DAEN). Fortunately, this now allows one to download sets of data based on filter terms. You can specify the COVID vaccines and you can specify particular “reactions”.
I downloaded a set, filtered on the term “myocarditis”. Note that there are other types of related heart problem eg, pericarditis, myopericarditis. So, I am only looking at records specifically with myocarditis and not covering all types of heart inflammation.
On this one term there were 1292 records, from start of injection rollout till 9 August 2022, when I did the download.

The shape of this histogram plot is what I was referring to at the start of this article. I had no preconceived idea of what results would be, based on this being a voluntary reporting system. It is known that reporting of adverse events has been discouraged in certain cases. However we clearly see the effect is worst for young boys in the 15-19 years age group. This is what is seen in overseas data.
The population of young men, ages 15 to 24, in Australia is 770,645 (for 15 to 19) plus 899,060 (for 20 to 24) = 1,669,705, from ABS data (Dec 2021).
I recall, from my reading, that it has been reported 1 in 5000 males in this age group, suffer myocarditis following vaccination. However there is a huge variation in the number reported in various studies. Assuming this population is 90% vaccinated (approximate value for Australia), then the injected population is approximately 1.5M. 1 in 5000 is approximately 300. In the graph above there are a total number of males, aged 15-24, equal to 157+89=246 reporting myocarditis following injection. So, the rate of myocarditis reported is consistent with reports from overseas of 1 in 5000. It is suspected that this is an underreported figure.
For the TGA reports of myocarditis, 1292 total, I made a count of the vaccine types identified.
Pfizer (Comirnaty) 1076
Astra Zeneca 77
Novavax (Nuvaxovid) 8
Moderna (Spikevax) 142
Not specified 128
These add up to more than the number of cases because sometimes more than one vaccine type is identified for a particular case due to the series of multiple vaccines delivered. Looking at the distribution of injection types from Health Department data (14 August 2022) we can see the rollout distribution.
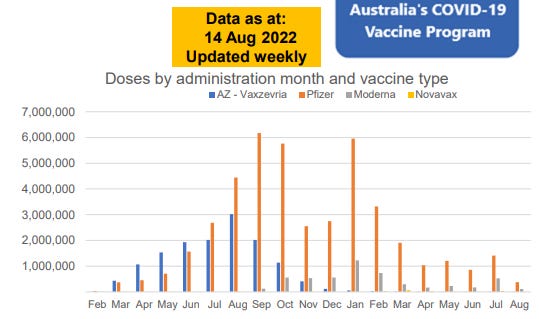
mRNA injections are by far the majority associated with myocarditis. However most young people will have received an mRNA type injection (orange bars) as AstraZeneca (blue bars) was phased out towards the end of 2021.
I have recently been looking through various Freedom of Information (FOI) requests to the TGA and Department of Health. TGA FOI’s are found here.
FOI 3545, dated 25 March 2022, contains an Excel spreadsheet with “COVID-19 adverse event reporting data”. Inside the spreadsheet is a big disclaimer:
The document released under FOI 3545 contains a list of batch numbers and ‘dose in series’ for suspected adverse events in people who received a COVID-19 vaccine. Dose in series is the reported location in an order or sequence for when the dose was administered, for example if it was the first, second or third dose of a COVID-19 vaccine received. The quality and completeness of the information is dependent on the data provided by the reporter.
The file contains one data row for each distinct combination of batch number and dose in series field values associated with a suspected/interacting COVID-19 vaccine in an accepted adverse event case created on or before 15 January 2022 in AEMS. Therefore, the extract contains multiple rows for a single case, where that case includes multiple doses in series.
Assessing batch safety on adverse event reports numbers alone is not expected to be a reliable indicator of safety. The nature of the adverse event reports would need to be considered, as well as other factors that may confound the interpretation of the data. For example, the size and/or distribution of the batch may influence reporting numbers as different batches may have been used in different populations, or in geographic areas which may have higher or lower reporting rates. To date, the TGA has not identified a safety signal indicative of a quality issue for any COVID-19 vaccine.
I have highlighted important points in bold. The FOI request only provides doses and batches up till 15 Jan 2022, so the myocarditis cases after that date will not have a matching record in this file.
Next I did a merge of the file with the myocarditis cases to look at which dose is associated with the adverse events. I widened the age group to 10 to 30 years to have a bigger sample size. The count of cases against number of doses is shown below.
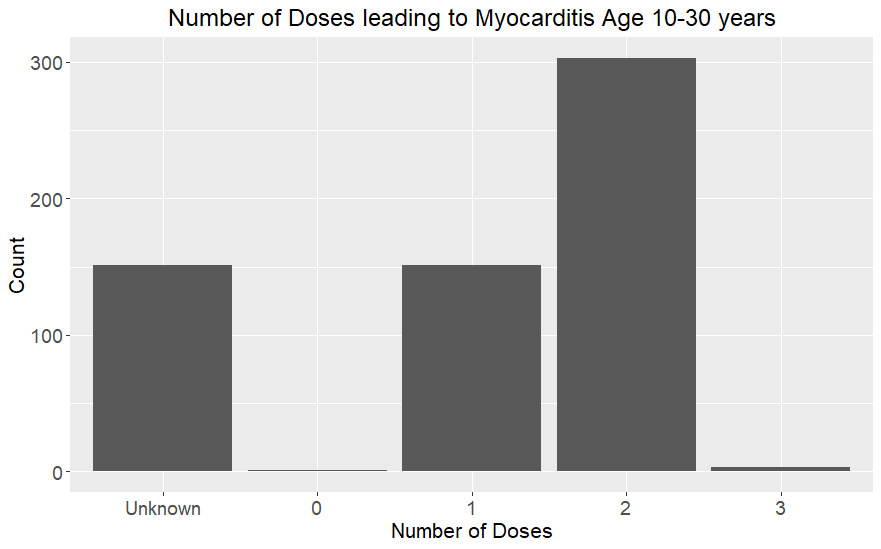
So this is consistent with what we know from other studies, ie that the second dose of mRNA is typically associated with adverse heart events. There are a significant number of unknown dose number. Some are because cases were after the 15 January date, others were just not recorded.
There was also information on batches associated with the cases, plotted below, for the same age group 10-30.
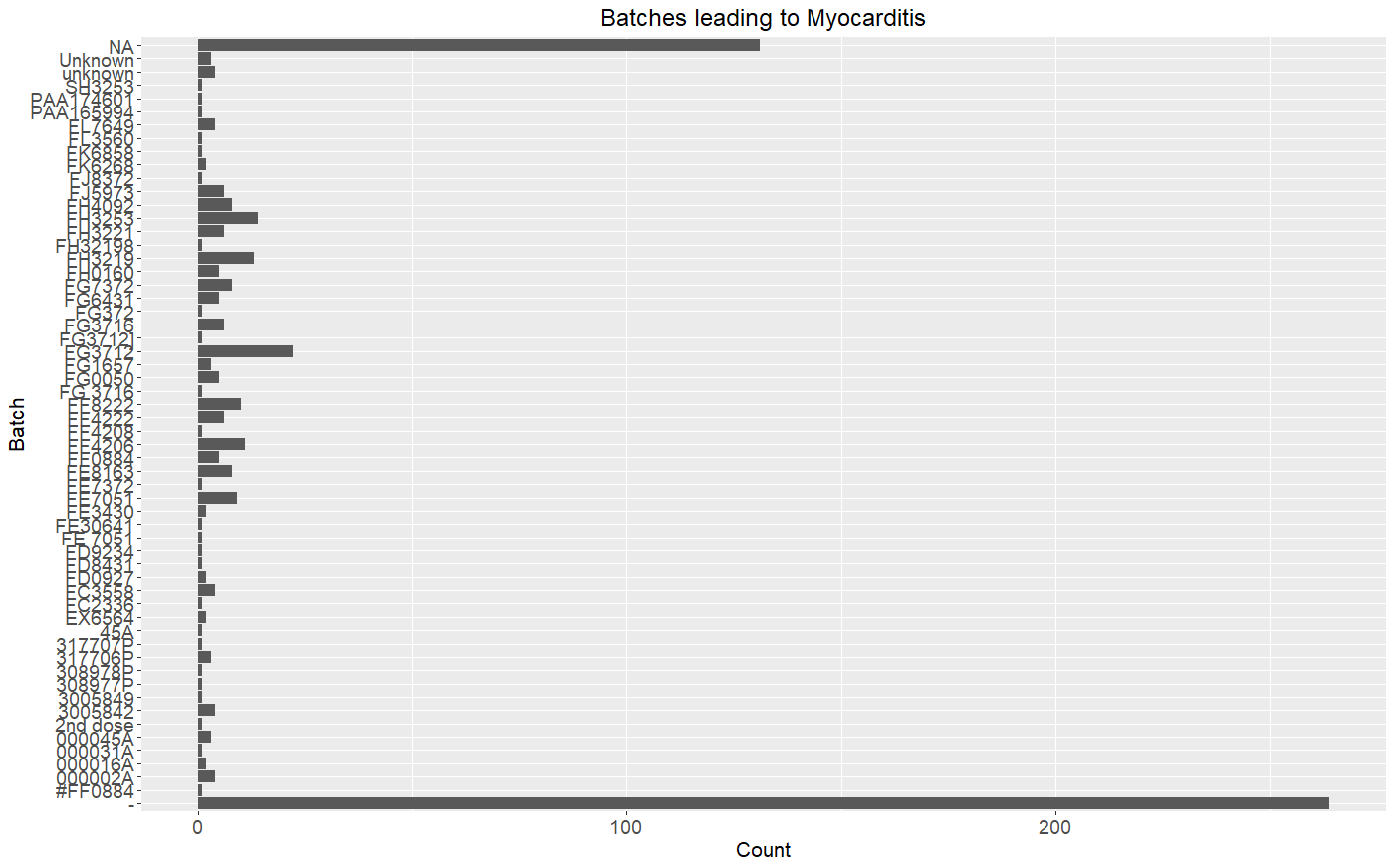
The batch names are likely too small if reading this on a phone but the majority are various categories of unknown: “Unknown”, “unknown”, “-“ and empty (NA). NA includes cases where there are not matching records after the 15 January date. The majority are dash (-) which means it wasn’t recorded. Of the named batches, one sticks out halfway up, FG3712. I filtered cases on this batch. Looking at the individual cases they all were reported from October to December 2021.
It’s not possible to draw any conclusion about a bad batch as it may be that this was a batch that happened to be in use around the time that the majority of young people were getting shots at the end of 2021, when strict work mandates were coming in place in Australia. Further investigation is required.
What is clear is that data recording is hopeless. TGA make the claim that:
Assessing batch safety on adverse event reports numbers alone is not expected to be a reliable indicator of safety.
Or course, with so many “unknowns”, it’s impossible to draw any conclusion on safety. In previous articles it’s been shown that unknowns are a way to confound any interpretation of data. The manipulation of unknowns in NSW Health data has been reported:
The only thing that should have been mandated during this time was integrity in data recording and reporting. It should have been mandated that any adverse event within a certain time period from injection must be reported with all relevant details filled out.
So the two lessons:
if you don’t want to know the answer to a difficult question don’t ask it and
if the question does get asked make sure there is sufficient uncertainty embedded in the data so that no definitive conclusion can be drawn.
I have watched quite a lot of Dr Campbell's videos and always found his analysis to be quite balanced with very little in the way of conjecture. Earlier this year I said to my partner that a sure sign of progress will be if Dr Campbell ever has a turn around on the vaccines. There seem to be more medical professionals joining this camp, Aseem Malhotra has also made some good commentary on the excess death phenomena in the UK;
https://twitter.com/DrAseemMalhotra/status/1559788722333310976
Another great write up. Thanks.