
Dr John Censored

After my article last week, on the Thai children myocarditis study, a friend sent me a link to a recent Dr John Campbell video on excess mortality. This is the link. But no need to click. To my surprise it showed:

He has been censored!
It got to 17,000 views on 20 August. A video like this would probably have got up to 1M views with his over 2M subscribers. Thank goodness for the wayback machine and web archives, I knew nothing about them before this age of censorship. I found it here on the wayback machine.
I meant to do a write-up on this straight away but I got scooped and several others have already written about this. It has also been uploaded on bitchute in case something doesn’t work with the wayback machine in future. But you don’t see the notes and links from the video there.
Basically, Dr John notes the excess mortality being experienced in the UK. More than 1000 extra non-COVID deaths per week above expectation. He then does the unacceptable by looking into reported deaths following vaccination.
It took a FOI request to the ONS get the number of deaths accepted by authorities to be from vaccination in the UK. It says 10 deaths are attributed to COVID vaccine. For comparison, in Australia with over 900 reported deaths following vaccination, the TGA website states:
The TGA has identified 13 reports where the cause of death was linked to vaccination from 931 reports received and reviewed. All deaths linked to vaccination as a likely cause occurred after the first dose of Vaxzevria (AstraZeneca).
There is a Vaccine safety report from TGA I hadn’t looked at before. Latest one is found here. There is a lot of downplaying of risks. For example for myocarditis it states:
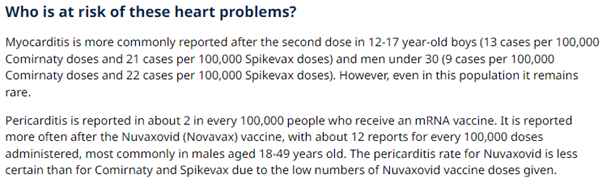
So the TGA comes up with a worst case of 13 cases of myocarditis per 100,000 for Pfizer and 21 per 100,000 for Moderna. Clearly this is a lot less than the approximately 2.5% seen in the Thai study and less than most other studies. It also says myocarditis is more likely following COVID infection. This is disputed by many. It also states:
Myocarditis is often mild, and cases usually resolve after a few days with treatment and rest.
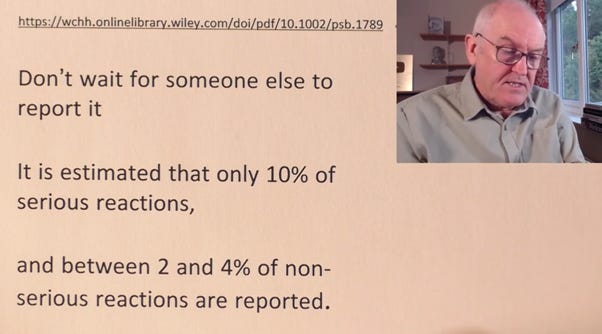
The UK Yellow Card system (equivalent of our TGA DAEN) indicates 2,109 deaths from Pfizer, Astra Zeneca and Moderna combined. Dr John notes that it could be less because of random temporal correlation, where a person just happens to die shortly after injection. He then goes on to point out the Yellow Card system itself says that serious adverse reactions to drugs are under-reported and requests people please report adverse reactions.

So his conclusion in the video is that deaths from vaccine in the UK could be anywhere between 10 and 20,000.
He says - Does this change the risk benefit analysis for vaccination? Clearly.
And boom, censored.
He has just today posed another video, not pulled down yet, triggered by the sad “sudden” death of a champion Scottish mountain bike rider who had won a championship a few days previously.
Events like this sad death of a prominent athlete raise public awareness and are impossible to ignore. When it comes to athletes things are more complex because they can be predisposed to adverse heart events. But in the UK there are now growing calls to investigate the excess mortality. This video may get pulled down as well.
Mark Steyn on GB News reports on excess mortality and the case of the Scottish cyclist. Steyn gets the message across with a much more sarcastic approach. It is very sad to see mountain bike rider Rab Wardell interviewed days after his win and looking happy and healthy.
The latest mortality data for Australia, up till May, was just released a few days ago.
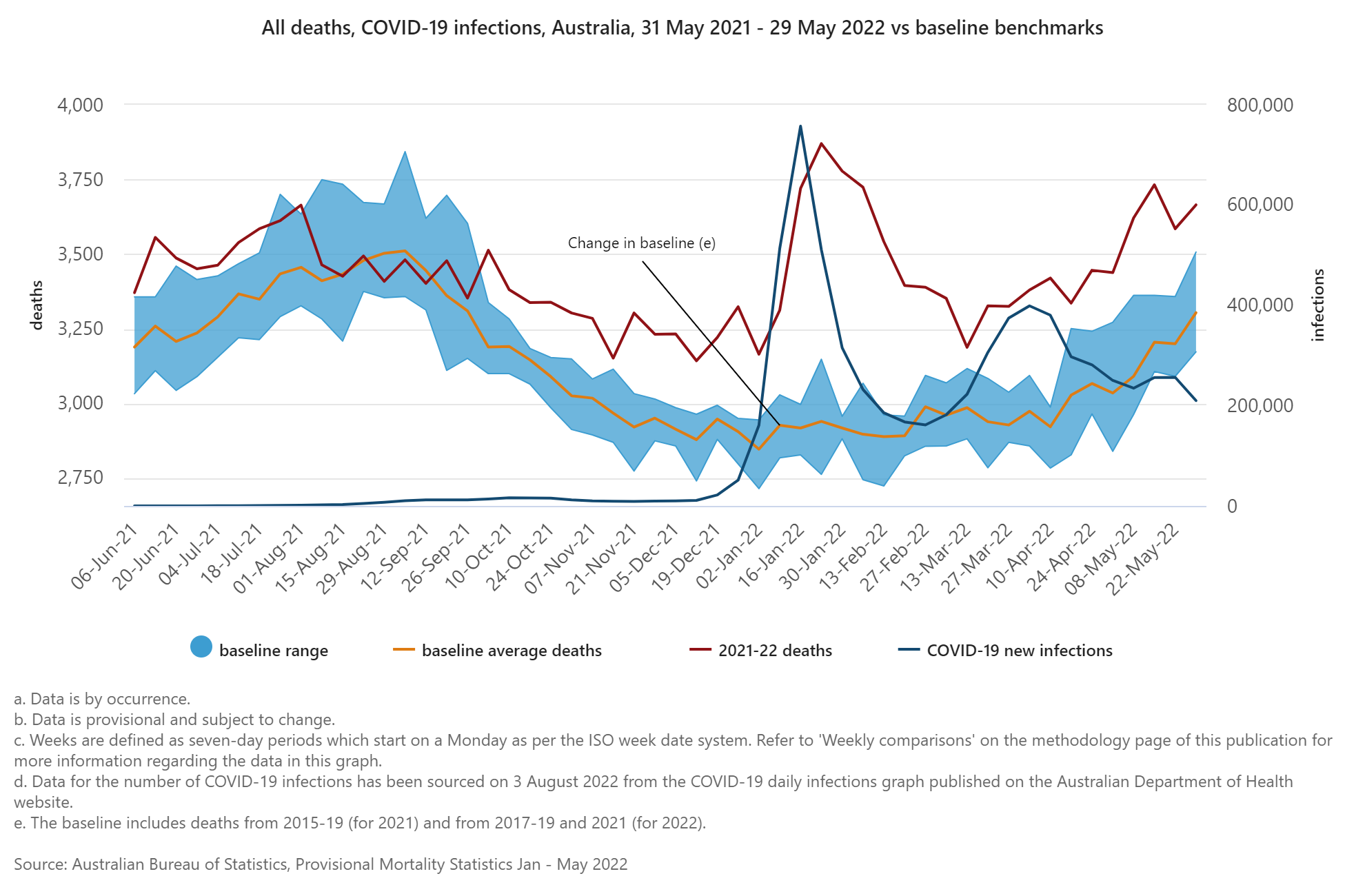
There is a continuing trend of excess mortality. Note that graph above is all ages and includes COVID deaths. I’ll have more to report on where I am up to on excess mortality soon.
There’s a lot more to dig into.
Final note:
As I was writing this article I was looking around for a document I had seen on Pfizer’s reported cases of adverse events. I recalled I had seen that for myocarditis the fraction of cases was something like 1% for the young age group. I wanted it to compare with the TGA reports. If anyone knows the document I mean, please post in a comment. I thought it was an Australian FOI request?
As I was searching I came across an Informed Consent Action Network (ICAN) FOI request to the CDC to get lot numbers and number of doses in the interest of investigating adverse reactions related to batches. The ICAN letters from Aaron Siri to the CDC are here and here. CDC response documents are found here. They are two spreadsheets I assume are in response to each of the letters. They have lot numbers and number of doses.
I had a quick look at the spreadsheets. In my previous article we found that a batch/lot FG3712 was associated with more myocarditis cases than others (about 20 cases). I did a search for that number in the ICAN FOI files. It indicates there are 24 doses in that lot. So that would mean just about every dose in that lot led to myocarditis.
However, I’m not sure yet if I’m understanding what is in the spreadsheets provided to ICAN. The lot FG3712 appears to be correctly identified as an international lot. I think the tabs are named in response to the ICAN questions (A,B,C). C1 is US and C2 is international. I found FG3712 on tab C2. However, some lots are shown to have one dose, which seems strange. But it’s something I’ll follow up. I’d appreciate anyone’s suggestions on this.
Thanks for another great right up. I Love the the quote in the Dr John video from Professor Heneghan,“The signals in the data suggest something is not quite right.” The Poms are the masters of understatement.
I’m surprised (not really) that there is no reporting of this information in the mainstream press. I guess it’s like you’ve said in your previous article, if you don’t look you can always say you’ve found nothing.
Hi Andrew. Can you please DM me. I am a FRNSW unvaccinated firefighter. Our union is taking the brigade to the Industrial Relations Commission in October to overturn the mandate. I have heard you have looked at data for RFS firefighters. Would any of that data be beneficial to our cause? Thanks.