

TGA Reported Vaccine Deaths in Australia
An Update

In my article Vaccine Deaths vs COVID deaths it was shown that for people in Australia under 60 there were more deaths reported as a result of vaccination than from COVID-19 itself.

COVID Deaths are shown over a background of Vaccine Deaths in Australia for the period March 2021 to Jan 2022.

The document containing ages of deaths from vaccination was obtained from a Freedom of Information (FOI) request made to the TGA. I note this is “reported” deaths and I make further comment on that below.
The Australian system for reviewing adverse effects is very clumsy, making it difficult to get this information out directly. It is called Database of Adverse Event Notifications (DAEN). This is the equivalent to the United States VAERS system. Hence the need to separately request specific information to understand what is going on. In this case someone did it as an FOI request.
The FOI response was a pdf document that looked like below:

I sought clarification from the TGA on the data provided in response to the request. Following the 28 pages with ages of deaths, the remainder of the 192 page document was completely blacked out pages which had led some to believe there were more deaths reported than actual.
TGA advised me the data provided in the pdf came from an Excel spreadsheet. Apparently, this spreadsheet was converted directly to a pdf and since the spreadsheet had more columns than would fit to an A4 page the extra columns (all redacted) appeared as additional pages.
It is bewildering that no effort was made to clarify this with the original response to FOI request. But what I learnt is that the FOI process is purely to provide an existing document in a redacted form, rather than provide actual data. I also learnt that the data was randomly sorted. Again bewildering. It’s as if there is an attempt to obscure information. What we suspect is that the ages will correlate with time of roll-out of vaccinations to different age groups. A sensible way to report would be to provide records in the order that they occurred.
I was also advised that there are apparently duplicates in this list of ages. They are not distinct cases. I assume a possible reason could be that a death is reported by multiple sources. The fact that no attempt was made to remove duplicates is astounding. It will of course make a difference to the data I presented in my original report.
At the time of the response to my inquiry, 24 March 2022, the TGA reported they had received and reviewed 792 reports of death associated with vaccination. Of these 11 reports only have been attributed to vaccination by the TGA. In my original analysis, based on the FOI document, I had worked on 921 deaths, 33 of which age was a null value. The null values are not in the bar chart. So there are 921 minus 33 = 888 death events in my graph. I was advised by TGA that nulls occur because apparently “age of the patient is not always available”.
I understand now there should be 760 deaths from vaccination (from going back to DAEN and counting from March 2021 to Jan 2022). So there are about 100 less deaths from vaccination than I have shown. However, the conclusion that there are as many deaths from vaccination as from COVID-19 for people under approximately 60, mandated to take the vaccine in order to be able to work or attend school in Australia, will still hold true.
Comment on “Reported Deaths”
I note that the TGA does not positively attribute the majority of these reported deaths to the COVID-19 vaccines. I understand that the small number of deaths that are confirmed (11) were attributed mainly to blood clot deaths from the AstraZeneca vaccine. So, these other deaths are presumed by the TGA to be the result of the random chance of people dying anyway.
However here is where I have a problem. A lot of the deaths occur in the elderly. In many cases the healthcare needs of the elderly are the responsibility of some other person, likely one of the children of the person. In Australia the term used is Enduring Guardian, for healthcare responsibility. An example where this is necessary is for people with dementia. The decision to vaccinate the elderly person may be the responsibility of one of their children or a friend.
So, imagine the situation where you, as the son or daughter, have to make that decision. It is clear from the graph above that with the COVID-19 vaccines, many elderly people are dying shortly after vaccination. In the graph above for the 80-90’s it is about a third of the number dying from COVID. The person responsible for approving delivery of the vaccine then has to live for the rest of their life knowing that they may have shortened the life of their loved one. This is tragic. Perhaps even worse is the case where parents make the decision for their children. We know there is negligible risk to the child from dying of COVID (unless there are some serious underlying health conditions).
A person approving delivery of a vaccine on behalf of a loved one needs to be able to make true informed consent. They need to know what the chance is that the parent will die tomorrow based on their age and existing conditions compared to the chance of dying of COVID (if they catch it) versus the chance of dying from COVID vaccination. It doesn’t matter that it is a going to be a “reported” death. They will be dead irrespective and we absolutely know a percentage of those reported deaths are caused by vaccination whether the health authority admits to it or not. The consenting person will have to live with that decision that they made. It will contribute to the legacy trauma caused by the pandemic measures.
For other medications and vaccinations we have comparisons of the likelihood of dying from adverse event reports for those medications. The COVID vaccination reports have to be viewed in the context of all other medicines. For example the elderly routinely get flu shots. The number of deaths reported following flu shots are orders of magnitude less than from the COVID shots. Jessica Rose, on her substack, has done amazing work looking into VAERS and other aspects of the pandemic response. In this article she looked at flu shots and COVID shots in the USA over the same period and found about twice as many (2.3x) covid shots as flu shots delivered. “We have 117.6 times as many reports of adverse events in the context on the COVID shots”. This is enormous. What this means is that these deaths reported from COVID vaccination cannot be ignored. If Flu shots are accepted as safe and COVID shots lead to over 100 times increase in adverse events, in my opinion there is serious question over whether they are safe.
These adverse events, reported for COVID vaccination, have to be taken seriously.
There have been calls for autopsies to be carried out on all deaths related to vaccination, which seems a sensible approach. While this may be traumatic for families involved, the importance of investigating the effects on the population of vaccination is of utmost importance. The costs would be negligible compared to the overall COVID pandemic costs.
I also believe the onus should be on the authorities to assume that the death has been caused by vaccination until proven otherwise, ie guilty until proven innocent. When human life is at stake this is the only ethical approach. Then the authorities have to make their judgement on the risk to benefit ratio of vaccination based on real data.
We know adverse events are massively under-reported. Jessica uses an Under Reporting Factor (URF) of 30. “If we use the actual number of deaths reported to VAERS which is 29,481 (this includes spontaneous abortions), the URF of 30 gives us 884,430 and a death rate of 1/1,000. 1 in 1,000 individuals injected will die.”
Comparing the US VAERS deaths data with Australia: Australia has a population of approximately 25M and USA 330M. US is approximately 67% vaccinated, Australia 84%. So therefore about 10 times more vaccinated people in the US. Australia therefore has a reported vaccination death rate of about half the US. However, this is still the same order of magnitude and so, given the uncertainties, is consistent. It is conjectured that in Australia there is more reticence to report vaccination deaths due to government control.
When it comes to COVID, if there is any chance the death is COVID related, then it goes straight into the statistics as a COVID death. There is an example from New Zealand of a man shot dead in his driveway, who later tested positive for COVID after death. This death appears in the NZ COVID statistics which seems absurd. Apparently, this is a WHO guideline on reporting.
I have mentioned the difficulty of using the Australian adverse event reporting system. Filtering on the COVID-19 vaccines from Pfizer mRNA, Moderna mRNA, AstraZeneca, Novavax (recently approved in Australia) and COVID-19 Vax (Type Not Specified), the number of deaths is, as at 11 April 2022, 820 deaths, increased from the 792 in my reply received from the TGA on 24 March 2022. I note that to date from the recent approval of the Novavax (non mRNA) vaccine (20 Jan 2022) there are no deaths reported, noting a much smaller number of doses delivered.
There is no obvious way to take into account the duplicates from the original data. We don’t know if they are spread evenly across all ages or maybe the ages occurring most commonly are the duplicates. I expect that they are mainly in the older categories. Accessing the ages of all the deaths from the DAEN directly is just about impossible using the website. They have disabled any ability to download the whole database of adverse events. You basically have to do queries filtering on a particular day, to get a manageable number, and look for the deaths. Death is not a medical condition listed so there is ambiguity working out the relevant cases to therefore find the ages.
A concerned person in Australia has set up a Telegram channel called “TGA Childhood Vaccination Injuries”. This provides reports of serious adverse events in children (up to age 17). They start in January this year. The author of the channel appears to have done this by filtering on each day and then manually looking through the cases with ages of children (one of the limited features is to sort by age). They have taken screenshots of what they consider serious cases and posted them on the Telegram channel. This is the latest one as I write.

This Telegram channel is a valuable resource given the difficulty accessing data from the TGA DAEN to use for analysis. I have scanned through this Telegram channel and in fact it helped me understand how to get information out of the DAEN from the way the author of the channel did it. I looked at one of the deaths of children reported and went back to the DAEN, on the TGA website, to confirm. However, to my surprise the particular case is not there!
The Telegram channel has a screen capture of the case reported, and several weeks later it is not in the DAEN. This is bad. If cases are being removed by TGA there should be some traceability. I have requested clarification from the TGA.
Perhaps there are mad anti-vaxxers entering bogus cases, but you would think that all the cases that appear via the TGA website have at least been reviewed. Certainly, if they have been entered by a medical professional or parent they must be maintained.
I see the post from Steve Kirsch today where he has a list of 43 questions he has posed to authorities. He cheekily states if he can get satisfactory answers to the questions he promises to stop being one of the top misinformation spreaders. See his question 10 regarding concern over cases gone missing in the VAERS. So, the same thing is occurring in the US with no explanation. The Informed Consent Action Network (ICAN) also has made a specific request for data from the CDC related to the death of a child that has gone missing in VAERS.
The Telegram TGA Childhood Vaccine Injuries channel has a summary of recent serious child vaccine adverse events found so far (Jan – April 2022) here. That post shows for example number of cases of heart attacks and myocarditis in children following COVID-19 vaccination.
The annoying thing is that there are statistical methods to quantify how likely these reported deaths are to be caused by vaccination, even if they are not attributed to vaccination from a medical analysis (or if the investigation has not been carried out). For every age an estimate can be made of the likelihood of death in the following period given no intervention. If the vaccine intervention was unrelated to adverse events we would expect the deaths to be evenly distributed over time from injection. This is not what is seen:

Jessica Rose finds the majority of deaths occur on day zero or one. I haven’t looked at the VAERS system myself but it is obviously a much richer source of data than we have available in Australia, to allow this to be extracted. Jessica Rose has also looked at another aspect. The graph below shows myocarditis following mRNA injection and which shot, ie 1 or 2. A presentation from Jessica, containing this slide, is in the video in this link.
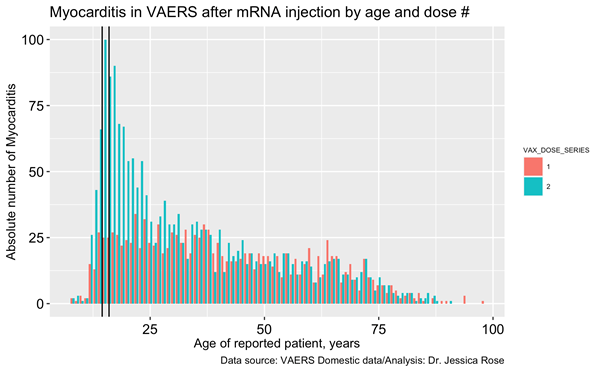
If the vaccination was unrelated to incidence of myocarditis there would be no difference between the shots. This graph is demonstrating a dose effect. The second shot is a sufficient dose to trigger the adverse event. It is clear this is the case for ages under 25.
I find the ingenuity of people digging into this data, when everything is being done to obscure it, inspiring.
Summary
In this age of big data and sophisticated analytics algorithms, where it is possible to do things like influence elections or purchasing behaviours, track individuals, etc, minimal effort has been put into creating quality publicly available data sources, other than to obscure signals which are relevant to healthcare.
Trivialisation by authorities of reported vaccine deaths is not acceptable.