
The Speed of Science

It’s been a while since I last posted. The reason is that I was asked to write scientific reports for a number of court cases here in Australia. These are being led by brave, honourable people fighting for justice.
I put all my technical ability into this, trying to be as unbiased as possible. Looking at all angles in available data. Unfortunately, I am unable work at the “Speed of Science” as apparently Pfizer did. For me science and analysis is painstaking and it takes time, you make errors, be honest about it and then fix them.
You would all be aware of the European Commission’s inquiry into the pandemic and on one day when Pfizer was in the hot seat, the Dutch member, Rob Roos, asked the question of Pfizer’s representative (CEO Bourla refused to appear) regarding evidence of protection of the shots for transmission.

This interaction will go down in the annals of COVID history.
I find the Dutch command of English is sometimes better than native speakers. “Please say it clearly….”
Of course, this is all a bit theatrical. It has been known since mid-2021 that the shots do not protect from infection and therefore do not stop transmission, as authorities promised. The whole basis of mandates was always flawed.
We knew this ourselves at the end of last year. Looking at data from the UK and New South Wales, which was how I started writing on Substack, showed Negative Effectiveness. Vaccinated people were more likely to be infected than unvaccinated. As soon as this became apparent authorities stopped reporting data where infections were categorised against vaccination status. Recent research papers confirm negative effectiveness.
I see in today’s news that CDC Director Walensky after recently getting her bivalent booster, thumbs up, has COVID.


So within a month she has COVID. There is the usual text with legacy media reports: symptoms are mild, will continue working from home etc…
In a tweet following, Vinay Prasad (UCSF Professor) writes

I will write further articles on the impact of Negative Effectiveness. Besides the “waning” there also appears to be a period immediately following injection where infection is more likely. I am seeing warnings in the data that if this is the case then vaccine campaigns in the midst of infection waves could be catastrophic.
As part of the reports I have worked on, I did a deep dive into recent NSW Surveillance reports. We have just been through our second major Omicron wave (around 80% BA.5). This saw a significant rise and fall of infections, hospitalisations and deaths. The peak was early August. These waves do not fall back to zero. Analysis of this period has provided insights into the dynamics of the process.
Many will be familiar with the dashboard created by twitter handle @LCHF_Matt found here: https://bit.ly/3ujYTQG
This excellent work has made NSW COVID data accessible. As part of my work, I checked all the data used in the Dashboard and I can confirm it is correct. I manually copied all data from NSW Health reports (with the help of my wife) and checked the vaccine data sources back to government data.
The only thing I would be careful of, is drawing conclusions on rates of hospitalisation and death of unvaccinated and 1 dose populations. That’s partly because these populations are small and because of the age distributions. Also unvaccinated people who die of COVID do not appear in hospital. To me this implies that they are people in aged care facilities, who are elderly and frail and most likely a conscious decision was made to not vaccinate. Others have different opinions of why this is.
For people under 65 there appears to be no unvaccinated people, who do not have significant underlying health conditions, who died of COVID during this wave. To be precise I could infer that the number was from zero to 3. People under 65 dying from COVID typically were vaccinated and had significant underlying health conditions.
In the following graphs I show, rates of hospitalisations and deaths for 2 dose, 3 dose and 4 dose, together the 95% confidence intervals calculated, seen by the strips around the lines.
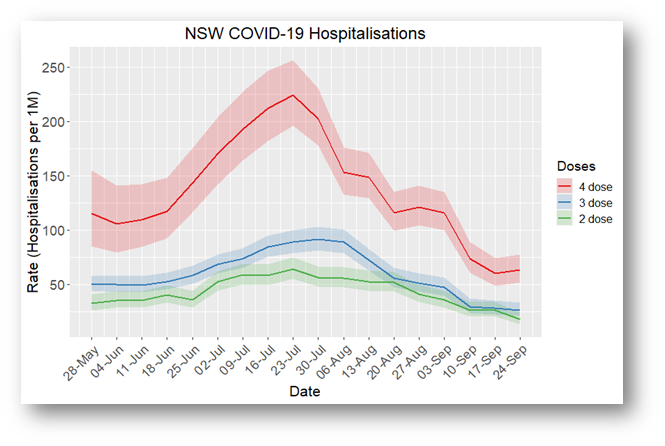
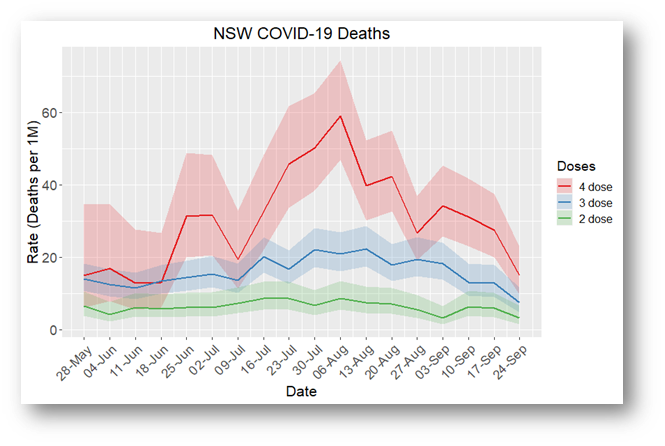
Now we have to be careful interpreting these graphs because the data are across all ages. Across the whole population of NSW, 2 dose people contains more young people, who do not die of COVID. The 4 dose people will be older and therefore more likely where deaths occur.
The government reports do not give us age together with dose status. I have made an estimate where I could of over 65 for one week and in that case I found that 3 dose was the worst.
But the most important feature is the sharp rise of the 4 dose. This is concerning. Have we done something that makes a particular group of people more susceptible?
Back to the European Commission. Dr John Campbell does a summary here:
See from 5 min 30 sec. The Romanian representative Christian Tehres is fired up. At 7 min 30 sec in the Dr John video, he suggests they should get their money back for:
“medical products that are not providing what they are marketed for”
The full Commission hearing is found here:
There’s much more to discuss, but I’ll finish this article with a recommendation to watch the interview on Epoch Times with Dr Joe Ladapo, Surgeon General in Florida
We watched it yesterday. There’s one really moving part in the interview. Jan Jekielek must be the best interviewer around at the moment. I’ve previously referenced one of the interviews in this series, he did with our Australian Economics Professor Gigi Foster.
Back now to working at the actual speed of science…
I’m a Qld lawyer representing (pro-bono) a young female copper (injured by the vax). I read your expert report yesterday for the QSC matter and on the back of that Qld removed some mandates. Just wanted to say thanks for all your hard work. From my side of things - there r very few of us. Because no-one is brave enough to go against the QLS cabal. But u wait...once these dam walls break these vultures will come out in droves.
Thank you Andrew for your dedicated work in this area.
You mentioned "Recent research papers confirm negative effectiveness." Do you know if that negative efficacy applies to anything the immune system needs to fight off such as a common cold ? If so, does the immune system show signs of recovering ?
Anecdotally I know more than a handful of C-19 vaccinated people who have caught 3 or 4 colds in the past 6 months when they would typically only catch 1 cold each year.