

Time to Death
A report by Dr Suzanne Niblett and colleagues on recent TGA FOI requests revealing time to death data for deaths reported following Covid vaccination

Dr Suzanne Niblett is one my colleague scientists collaborating with the Australian Medical Professionals’ Society (AMPS). She contributed a detailed chapter on Adverse Event reporting in Australia in the AMPS submission to the Excess Mortality Inquiry. The AMPS full submission (pdf can be downloaded here) was one of those not uploaded to the government portal for the public to review.
She and other team members have been submitting FOIs to the TGA, to glean relevant data to analyse the safety of the new medicines, which unfortunately is the only way to obtain it.
Her report, on Time to Death data, released today, authors Dr Suzanne Niblett, Leon Anderson, Andrew Madry and senior author, cardiologist, Dr Chris Neil, can be downloaded here:
Arduous pursuit through FOIs has recently obtained a table with the time in days from vaccination to death for all the reported deaths in the DAEN.
The number of deaths that occurred on the day of injection (35) and within 3 days (184) is alarming.
Unfortunately, we are not yet able to reference ages of those deaths or the medical terms related to the deaths, from the data that has been released. However, what has been obtained is still very important data. Dr Suzanne has done a deep dive into the data and to review it in full please download the report using the link above.
In this article I will provide a summary, my own impressions of what this data means and some observations related to all-cause mortality.
The reason this data is important is that currently the TGA accepts that only 14 deaths are causally linked to Covid vaccination. There are currently 1042 reported deaths in the Database of Adverse Event Notifications (DAEN).

Graph top shows number of deaths, the month they were reported, from Feb 2021 (rollout started right at the end of Feb 2021), and bottom right the age distribution.
Summary of the FOI 25-0047 data
Of the 1037 reports of death (at the time of the FOI), 771 reports had time to death available. This leaves 266 where the time was not available
184 (24%) died within 3 days of the vaccination.
35 people died on the day of the vaccination.
Number of deaths reported for the first 7 days:

My initial observations
That 266 reported deaths do not have important fields available, such as the time to death, is astonishing. One would think that it would be someone’s job at the TGA to go through each report and contact the relevant reporter and/or family. Note that we know that in 73% of cases the report was made by a health professional (Dr Suzanne’s report details this from other FOIs). When I worked in a major hospital cardiology department, early in my career, I shared an office with a lady whose job it was to ring up every patient following a major procedure at specified follow-up dates. There were occasional awkward conversations I overheard when the patient had passed away in the interim and a family member answered the phone. Nevertheless, everyone was followed up.
That the TGA does not have the information, for such a large proportion of the reported deaths, appears to be negligence. The same is true of batch numbers. Using OpenDAEN you can also cross reference batch numbers for all the adverse events including death. Apparently, we know from Parliament (Question on notice no. 250, Portfolio question number: SQ23-000281, 2022-23 Supplementary Budget estimates) that the Batch number is not a mandatory field. One would think that a professional pharmacovigilance system would chase down the batch number of every serious adverse event reported.
35 people died on the day of injection,
ie day zero. This means it could have been literally hours from injection to death for these 35 people. The number that died within 24 hours of injection is therefore somewhere between 35 and 87. Clearly the TGA claims these are coincidental deaths, given only 14 are accepted.
We know that many of the reports of death occurred early in the rollout. We know that the majority of the deaths are in the older population. So, it follows that many of the deaths occurring in a short time frame after injection are in the older population.
However, the TGA does not allow us to determine this unambiguously. They use “privacy” concerns as a mechanism to avoid releasing the relevant data. In FOI 25-0093 the case numbers for the Time to Death data was requested. The response provides the case numbers but sorts them numerically so there is no way to match them up to the list in FOI 25-0047. Obfuscation has become an art in these agencies. No clarification of this is provided in the FOI disclosure log and it will lead people falsely making that inference.
As an aside, for a chuckle, Professor Carl Heneghan and Tom Jefferson in their “Trust the Evidence” substack today (Jan 13) write an amusing letter to the UK equivalent agency regarding obstruction using FOI responses.

Well worth a read. The agencies behave similarly around the world.
The Risk to the Elderly
The risk to the frail elderly was known early on in the worldwide rollout. In January 2021 reports came in from Norway that a large number of elderly had died shortly after injection the Pfizer vaccine. This was months before Covid vaccines were available in Australia.
A short video on Sky News from January 2021:

The Health Minister at the time Greg Hunt makes an appearance to reassure the public.

He states: “A function simply of age and people who are older who sadly facing the natural loss of their life or whether there is any causation, and that hasn’t been asserted as yet.
But we are proceeding with an abundance of caution … the medical regulator is completely empowered….”
To paraphrase: old people die anyway so don’t worry about it, we are rolling it out irrespective.
Of course, the clinical trials only enrolled young healthy people so we knew nothing about the safety risks to the older population. I recently came across this video on excess mortality in Germany where the presenter points out that when they analysed the death rate during the clinical trials, based on the ages of participants, that it was far less than expected for the general population. In other words, they were biased to be a very healthy trial group.
A crucial ethical point
I have found it difficult to express clearly what I believe is a crucial ethical point. I’ll try again here.
When it comes to risks for the frail elderly, extreme, extreme care needs to be taken. The notion, expressed by the Health Minister, that they will die anyway, is dangerous. Performing some intervention, of any kind, could very likely hasten their death. Operations are often not performed on frail, elderly because the risks often outweigh any benefit.
There were no randomised controlled trials for this demographic and we are relying on the TGA, who we know does not follow up adverse events thoroughly, to determine if it is safe. This is terrifying.
Detecting the safety signal is difficult because of the increased likelihood of death as age increases. We can’t use annual excess mortality as a measure. If someone is likely to live for a few more months and they are given a dose and their life ends prematurely we don’t detect that in annual numbers. Typically, they will have died in the same year. The deaths caused by evil Harold Shipman (see substack by Dr Ah Kahn Sayed on Shipman) wouldn’t appear in excess mortality numbers.
My report in the AMPS submission to the Excess Mortality Inquiry (Chapter 5) made estimates of the excess mortality in Australia up till the end of 2023. Rounding the numbers, approximately 40,000 excess deaths of which approximately 20,000 were not directly from COVID.
If there were premature deaths of elderly, caused by injection, where their death was anticipated within the next year, these numbers do not contribute to the cumulative excess calculated. They are effectively hidden. This is a point that bears consideration. In actuarial terms it may be only person-months of lost life but these are real people with families who would have treasured every extra day.
There are many reports of death immediately following injection. Dr Suzannes’s report provides a thorough analysis of the information obtained through FOI. She discusses under-reporting factor, which is well established for passive pharmacovigilance systems. Of course, in the Covid era authorities claim there is over-reporting to pharmacovigilance systems. She references that. She analyses the medical terms associated with the reported deaths. The most common term is the generic: “Adverse Event Following Immunisation”. Of note is the second most common term which is cardiac arrest.
Someone has submitted an FOI requesting all documents related to the generic term.

The TGA must have worked overtime to get the response out the day before Christmas. You would have run out of black printer toner over the Christmas break if you decided to print this document out. It is basically a document of blacked out pages.
This may be a good point to wrap up this piece but I have some more for those who want to dive a bit deeper into the data.
Part 2
As I reflected on Dr Suzanne’s report many things occurred to me with respect to the areas I have focused on. This is the benefit of a multidisciplinary team working together including medical professionals in AMPS.
I was trawling through various Senate hearings, to understand what was known at different times.
There have been several important Senate Hearings in Australia, where the few honest politicians who do their job, have probed for answers from health authorities. One of them is Senate Committee Meeting 10 November 2022. Hansard record is found here (helpfully uploaded by a member of the public).
There is an interaction between Senator Rennick and head of the TGA, Dr Skerritt found on page 53 of the transcript.

A couple of key points. Senator Rennick is asking about the increase in deaths seen in 2021 in the older population. Skerritt claims there is no correlation between date of death and date of vaccination. This doesn’t actually make any technical sense but let’s go on.
Dr Skerritt: The ABS statistics have not been seen by any of the professional group such as the actuaries, who make a living out of doing this, as being associated with vaccination.
This statement is astounding to me. Remember the TGA is supposed to be responsible for safety of new medicines. First there is deflection to “ABS statistics”. Then “any professional group”. They certainly didn’t ask the professionals of the Australian Medical Professionals Society. Then it is the nebulous “actuaries”. Of course there is a Mortality Working Group of the Australian Actuaries Institute who have produced reports on Australia’s excess mortality. As I understand it, they have no interaction with medical professionals. I lost all respect for any of their reports because when it came to looking at causes of the non-Covid excess, which can be underestimated, but can’t be hidden, they included in a list of possible causes, deaths from vaccination but disregarding it as non-significant for the only reason that the TGA say there are only 14 deaths causally related. I say this, not because I dispute the TGA’s 14 deaths, but because the actuaries did no analysis of the TGA DAEN and blindly accept this number because government says so.
Can you see the circular arguments here? TGA say there is no excess due to vaccination due to the actuaries analysis and actuaries say there is no excess due to TGA analysis. Neither have done any detailed investigation. In our AMPS multidisciplinary collaboration we have some actuaries contributing and they are disillusioned with the Actuaries Institute for a range of reasons. In Australia we don’t have to look far for a scheme run by actuaries where budget has blown out of proportion such that it is now necessary for government to hide reports.
I am quite proud to be involved in the AMPS multidisciplinary collaboration which goes beyond what these other organisations have been doing.
In Senator Rennick’s interaction with Dr Skerritt he goes on to ask him about his previous claim that lipids in Lipid Nano Particles are like what we find in a breakfast sausage (I refuse to eat sausage at breakfast anymore).
In another interaction Senator Rennick posts here:

The head of the TGA claims:
more than 10 times as many people have died from paracetamol than adverse events from Covid vaccines.
I think he means specifically deaths from Covid vaccines. Of course it is nonsense. They must hope that no-one will check up on this. Senator Rennick did. In the notes for the video from Jan 2021 to Feb 9 2023 there were 50 reported deaths for paracetamol (with one listed death from the Panadol brand solely); 24 deaths were overdoses including 10 intentional. The 26 remaining do not list paracetamol as the only drug taken.
This is our medical regulator. Too many breakfast sausages followed by Panadol.
The Child Deaths
Someone referring to themselves as “Swollen Pickles” has helpfully collated important segments from Budget Supplementary Estimates 2022–23, Community Affairs Legislation Committee, Department of Health and Aged Care, 16 February 2023.
At the 5:20 mark (linked) Senator Alex Antic raised the question of cardiac arrest in two children ages 7 and 9 following Covid vaccination. TGA claims they don’t have much information. “Unfortunately they were not able to get sufficient information on these particular cases…..”
One would think that no stone should have been left unturned in this situation. It is admitted that the deaths are closely temporally related to vaccination. We suspect the children were not on the sports field.
Apparently, an expert external panel with at least one doctor on it reviewed these cases. We don’t know if there was a cardiologist involved.
At the 7-minute mark Senator Alex Antic continues questions about the deaths of the two children from cardiac arrest. Further information on these deaths had been found out through FOI by Dr Melissa McCann and the indication was that the internal committees reviewing these deaths considered whether they were causally related. According to the TGA testimony they were not considered causally related and therefore not part of the 14.
At the 6-minute mark in the compilation Skerritt claims that “heart attack” is not a known adverse event related to covid vaccines. In Dr Suzanne’s report the medical conditions related to the deaths are analysed and cardiac arrest is the second most common after the generic term Adverse Event Following Immunisation. Myocardial Infarction follows closely in numbers after Thrombocytopenia.
So how he can say this is unfathomable.
I note we have to be careful about the term heart attack. This is a more colloquial term that does not specifically appear in the medical terms. Heart attack is technically Myocardial Infarction. There is a difference between myocardial infarction/heart attack and cardiac arrest.

Senator Antic asks “How often do 7 and 9 year olds die of cardiac arrest?”
Dr Skerritt claims “…it is not as uncommon as you think, something like 100-200 deaths occur due to sudden cardiac death on the sporting field”. He admits though that they are typically teenage or in their 20’s.
Again, it’s the people die anyway argument. These two child deaths, that we know from the discussion occurred close to the date of vaccination, were just coincidental bad luck. Nothing to see.
Senator Roberts chimes in, referring to FOI 3727, the discussion gets heated and the Chair decides at 10:30 mark in the linked recording to quickly cut the feed: “the committee suspends, the broadcasting is off”, presumably the public doesn’t need to hear any more.
You can’t make this stuff up.
Searching back through legacy media reports of deaths, this one from legacy ABC news appeared in April 2021.

It reported on two NSW men who had died of blood clots and the families had said they were perfectly healthy prior to vaccination. This report is from April 2021 so very early in the Australian rollout. Skerritt makes an appearance in the clip and says that these men had clotting disorders so the vaccine didn’t cause it.
What?
It’s like saying if we give peanuts to a person with a known nut allergy and they die it’s not the fault of the person supplying the peanuts.
I’m starting to ramble here but it is quite instructive to analyse these interactions and reports. It’s sifting through signal and noise.
The TGA will find it hard to replace the master of noise generation.
Finally….
Finally, back to my own area of expertise which is signal processing. Very often it is in the noise that we find critical information.
I have noted that the deaths of the frail, elderly that occurred a short time-frame after vaccination are difficult to detect excess in annual numbers but we can detect it in the time domain data. From my Chapter 5 in the AMPS excess mortality submission, I refer to two graphs reproduced below. There is a random component in the week-to-week deaths that occurs. We can look at the difference in week-to-week deaths in Australia. This is superimposed on the seasonal pattern and overall trend of mortality numbers. From week-to-week deaths go up sometimes and down sometimes. Typically, this week to week change stays within some bounds. It is affected slightly as the season changes.
This week to week difference is shown, from 2015 to 2023, in the graph below.

There are clearly two outliers occurring in 2021 and 2022. The biggest one occurs in January 2022. This is when a confluence of events occurred. Borders had opened up to vaccinated travelers, bringing with them the Omicron variant. The population had reduced immunity due to being locked down for so long. Lockdowns were relaxed and people started going out again. Boosters were at maximum rate of uptake. For the elderly population the time since primary vaccination was over 6 months. We know there is a susceptibility in the immediate period following injections. So Covid hit Australia hard. We had the highest infection rate in the world at that time.
It is the first outlier, that I have circled in red, that I refer to. This too is way outside the normal difference in deaths week to week. There was no Covid and minimal influenza in Australia at this time (second week of April 2021). Why would there be such a change in the pattern of this signal at this time?
I think we know the answer. Looking at another graph from my report, taken from ABS data, specifically for the State of Victoria.
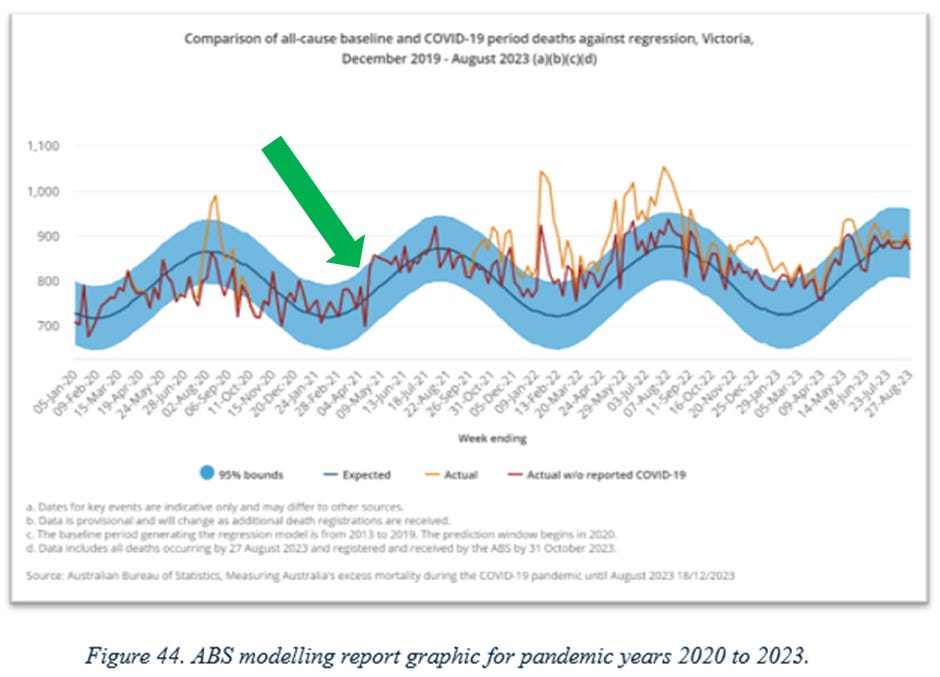
Draw your eye to the feature of the pattern I have indicated with a green arrow. Something never experienced before, ie a jump in week-to-week deaths, of the order of 100’s above what might be expected, happened in Australia at this time. No amount of sausages, Panadol or deaths on the sports field can cover it up.
Healthy Vaccinee Bias
If we were to give the whole population some benign intervention and we studied the time to death from this intervention we would expect roughly a constant number of deaths from the time of the benign intervention to the time of death across the whole population. It is affected slightly by the actual time of year due to seasonal effects, but roughly constant. People would randomly die close to the time of the intervention.
But it is very different for a medical intervention. We know that deaths should not occur in close proximity to the time of vaccination. Those frail elderly or cancer patients, known to be close to death should not, in good conscience, be given a new medicine.
This is called the “healthy vaccinee bias”. People receiving the vaccine should in general be healthy.
There is rare, publicly available data, to assess this, as population mortality data and vaccination status is closely guarded in all countries. The New Zealand data leak (refer here and here) and Czech data gave some insight. All cause mortality in the days close to vaccination is much reduced from the overall average level. It should be rare that someone dies close to time vaccination. Of course, they could walk out of the vaccination centre and get hit by a bus, which could be a random event but even then, if a person gets dizzy and falls into traffic then it is not a random event. So, all deaths close to time of vaccination need to be carefully investigated. Not just those that are specifically reported as being caused by vaccination. Authorities appear not to be doing that and if they are they are not making the data available.
These deaths, occurring within a few days following Covid vaccination, that have been obtained through FOI, and possibly under-reported are important to understand the safety of the novel medicines.
Congratulations to Dr Suzanne Niblett and colleagues for this important work.
And best wishes for the New Year to all readers of Data Wise.
Dr Suzie Niblett and Dr Andrew Madry will, I hope, one day get AMs for all their work throughout the covid years in Australia. This piece of work spearheaded by Suzie typifies her dogged pursuit of truth.
Andrew, with his extensive knowledge of the political fight by brave Australian politicians over the covid years, has produced his usual interesting and very readable summary of Suzie’s work, laced through with relevant video clips. He always makes me laugh out loud at some point.
In 2019, working as a medical journalist, I respected and trusted TGA and ABS announcements. I no longer trust these agencies. We need an independent and transparent examination of every death reported to the TGA as being potentially linked to covid vaccination. Every family should have been contacted by the TGA and should have received a personal visit, with no stone left unturned in trying to ascertain the actual cause of these deaths.
A fantastic analysis, much of which any interested layperson could understand. The data are already damning, and the longer the government delays a Royal Commission, the more evidence there will be against this technology. The government would do well to get it over and done with in my opinion.
They’ll be an almighty rumpus I think should any new across-the-board mandates occur in the future, much like the London poll tax riots back in the 90s.