Vaccine Effectiveness across the World

Fact checkers are working overtime to explain away the overwhelming real-world evidence that those vaccinated are more likely to be infected with COVID-19 variants than those unvaccinated. We are hearing of those boosted being infected multiple times within a 6-month period (eg White House Press Secretary Jen Psaki). The reasons for decrying reports of Negative Effectiveness include that you can’t use the surveillance data, effectiveness has to be measured in a controlled trial. However we already know that performance of these products in any industry sponsored trial are always going to be promised to be better than what is ever found in practice.
Another reason is that the unvaccinated can’t be trusted to be tested.
I reported, in my first article on UK data on how the narrative provided with surveillance reports was adjusted as numbers went the “wrong way”. When we look at infection rates in unvaccinated versus vaccinated across age groups, it’s consistent across countries.
The recent “Digger podcast” hosted by Phil Harper, with guest Professor Norman Fenton, is a good discussion. Professor Fenton gives an overview of his work. He uses a Bayesian risk based approach to analyse data. During the discussion Professor Fenton notes:
“There’s nothing to suggest a positive correlation between the COVID mortality and lack of vaccination … there’s no correlation at all. There’s no relation ... Wherever you look for the evidence you can’t find the evidence to support vaccination being effective. And yet wherever you look for the observational evidence for Ivermectin, not the randomised controlled trials….”
Thinking about how to look at data in a different way to get an alternative perspective on vaccine effectiveness I thought it would be worth looking at the vaccine performance across different countries myself. One of the things I like to do when I hear of some reported trend is to be able to reproduce it myself. That’s a good test. If multiple people get the same result, perhaps looking at it a slightly different way, then that’s supporting evidence.
In the podcast Professor Fenton notes the issues and confounders with the “Our World in Data” site. I also found that in my work here. For example, I found vaccination rates reported were different to Australian government sites. Numbers of Infections and Deaths also varied. This is understandable to some degree. The Our World in Data site is an amazing resource and big effort to collate all the data from every country.
However, we don’t have access to this data, for all countries, with both deaths and infections, for vaccinated versus unvaccinated, and across age groups. But it is worth looking anyway to see what we can find.
Pre-processing the data took a long time. There are gaps in data in various countries. I removed countries with very small populations. We cannot rely on data from some countries (eg China) so they were removed.
Also, I first looked at infection cases but found that it is likely that this is not measured accurately in some countries. Deaths on the other hand are likely to be more accurately represented.
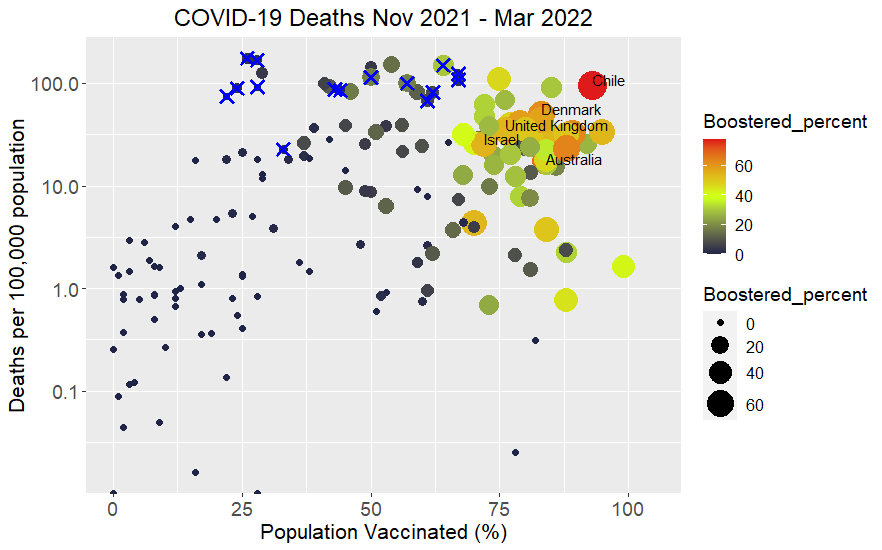
Here’s the result for COVID Deaths:

There is a lot of detail in the graph and I hope substack keeps the resolution if you download the image and expand it to inspect. It will be hard to see the country names on a phone. I can send the png file for those interested.
I used the period from 1 November 2021 to the day I downloaded the most recent Our World In Data dataset (26 March 2022). The Omicron variant officially came into existence from 24 November 2021. But it was probably around before this. The idea is to look at infections and deaths over this period and compare that to vaccination rates for different countries.
The horizontal x axis is the percentage of population vaccinated. This is presumably the percentage of total population that has had at least two shots. Note the outlier of Gibraltar, with a percentage greater than 100%. That has been reported in the news due to a large number of temporary workers required to be vaccinated that were included on top of the residing citizens. So, for all intents and purposed it is 100% vaccinated.
The vertical y axis is the total deaths over the 5-month period per 100,000 of population. For Australia there have been approximately 4100 COVID deaths over this period (that’s about 6% of the total of all deaths for the previous year). With a population of 25.8 million that’s approximately 16 COVID deaths per 100,000 of population. I also looked at the maximum found over the period. The trend was similar.
I have made the y axis a logarithmic scale. It’s a bit hard to see the trend on a linear scale, eg a lot of countries sit close to zero and the Eastern European countries have higher death rates(more on Eastern Europe later).
I have sized and coloured the points according to the percentage of population boosted. I used a colour scale that starts as black/dark for small percentage boosted ranging through green, orange and then red at the maximum (around 80%). Chile hits this mark.
There is a clear trend displayed in the graph. There are many countries with vaccination percentage less than 40% that have a low death rate. The overall trend is that the higher vaccination percentage of the population the higher the death rate.
Of course, it’s not that simple. This data is for all ages combined. The countries up the top right are all wealthy countries and have older populations. COVID hits the eldest the hardest. If you look at the age distribution for African countries it is very skewed to younger ages. See this paper titled: “The Conundrum of Low COVID-19 Mortality Burden in sub-Saharan Africa: Myth or Reality?”
Of course, it has to be a “conundrum” because of the low COVID vaccination rates. There is a comparison in the paper of the age distribution of Uganda and Canada, showing how distinct the difference in ages is. So my graph above could also be showing a trend related to age of population. However, vaccination clearly isn’t doing much to help that. I think it’s also interesting to look at the effect of boosting amongst the wealthy countries.
The Our World in Data also has aggregate data for what it terms: Low Income, Lower Middle Income, Upper Middle Income and High Income countries. That trend is interesting… I’ll leave it to you what that shows.
In the podcast referred to above they discuss work which looked at sub-Saharan African countries where Ivermectin is used prophylactically to treat a disease called river blindness. This was compared to similar demographic African countries where Ivermectin was not used and apparently there is a distinctly lower rate of COVID deaths in those countries where Ivermectin is used. Another conundrum.
In the top middle of the graph there are a bunch of countries with a high COVID mortality. Vaccination ranges from about 20% to 70% in these countries. If you inspect closely, you will see that they are primarily Eastern European countries. In the graph below I have taken the names off the points and put blue crosses on the official Eastern European countries. Croatia, Serbia and Bosnia, not strictly Eastern Europe, are also in this region of the graph but are not crossed. What could be the reason for these high rates of death?
Looking at the trend over the period for individual countries it is found that there is a peak of a wave prior to Omicron. See graph below for Bulgaria:

By including November in the total this is probably biasing the result, aimed to be for Omicron only. All the Eastern European countries show a tail of death from a previous wave of COVID prior to December. Of course, it is Winter in Europe at this time and there are always a lot of deaths due to Influenza during this period. Anyone who has experienced an Eastern European Winter can attest to it’s harshness, particularly on the poor or elderly.
For comparison see the same graph for Australia where the was almost no COVID prior to Omicron as we came out of severe lockdowns, particularly for unvaccinated. The Omicron peak was in January. I caught COVID myself at the end of December.

This graph displays a classic shape seen in many of the wealthy countries. There is a peak in infections and two weeks later a peak in deaths. For Australia there is approximately 1 death per 1000 infections. But watch the rate of boosters and infections rising again.
See also for Israel:

Boosting appears to have leveled off in Israel. The Omicron peak is a little bit later than Australia and there may be an uptick just starting at the end of March. We know Israel are on their 4th and 5th shots but data does not indicate whether the booster number incorporates first or second booster (eg do boosters add cumulatively to the per 100 number?).
The rate of infections and death is about twice as large as Australia. How can this be? What is the difference. Both are wealthy countries with similar demographics…
Going back to the original graph, or the one I have taken most of the labels off. Eyeballing it and following the ball sizes/colours it does look like boosting is not doing anything to improve the situation.
There are some boosted countries with lower death rates. They include New Zealand, which has only just come out of lockdown with rates of infections and deaths now starting to increase rapidly from the end of February. Bhutan: blocked to tourists until recently, 2-3 week quarantine still required, United Arab Emirates: the current Australian travel advice warns that there are missile and drone attacks so there may not be too much tourism going on! So these countries are likely not yet showing any effectiveness of vaccinations.
Taiwan shows a very low death rate on the original graph. They are still in a COVID-zero policy, so there is no demonstration of vaccine effectiveness there.
Final Thoughts
The Our World in Data site notes, in text that has probably not been changed for some time:
“To bring this pandemic to an end, a large share of the world needs to be immune to the virus. The safest way to achieve this is with a vaccine. Vaccines are a technology that humanity has often relied on in the past to bring down the death toll of infectious diseases. Within less than 12 months after the beginning of the pandemic, several research teams rose to the challenge and developed vaccines that protect from SARS-CoV-2.
Now the challenge is to make these vaccines available to people around the world. It will be key that people in all countries — not just in rich countries — receive the required protection.”
The World needs to pause and start thinking...
The poor countries seem to be doing OK, so long as the rich countries keep out of their business. The rich countries have to work out why vaccines are not stopping infections or death. They have to look at the “all-cause mortality” and confirm that we have not increased that at the expense of saving some other deaths. The trajectory observed from bottom left to top right of the graph, shown here, is concerning.
Thanks Andrew. Very interesting and it backs up what I have always thought that the vaccines are no way doing what Big Pharma said they would. I have shared the article on twitter so will be interesting to the comments. Cheers.
Similar work from France: https://twitter.com/felicittina/status/1506644148329320449