

Excess Dementia Deaths in Australia
"For every complex problem there is a solution that is clear, simple, and wrong"

This article is a bit of a journey. It leads to what appears to be a mortality event in 2021, unrelated to COVID. It wasn’t what I expected when I started this analysis. There are lessons for healthcare. For those following the investigations in the UK to the COVID response with Matt “deploy the variant” Hancock, the incompetence of bureaucrats and politicians is relevant.
Over the weekend Steve Kirsch posted an article on some inside information he received on deaths in an Aged Care facility in the state of Victoria, Australia. Apparently 24 people died in less than a year (Sep 2021 – Aug 2022) in a 114-bed facility, when a smaller number is expected based on ages. Kirsch estimates the number is 80% above normal.
There are almost 500 comments to the article. There is discussion on how many people would be expected to die in a year in an aged care facility. There are many factors to consider, eg type of care (high/low), demographics of the residents. If you scan through the comments there is a reference to an aged care report from British Columbia, with useful data in it.
This raised the question for me, of how many people do we expect to pass away in aged care facilities? Can we look at that trend over time in Australia? How has the response to the pandemic affected mortality?
In this substack we have sliced through mortality data categorised by age, state and number of doses of vaccine. We saw the signal of non-COVID excess mortality start in 2021 in Australia.
But what about where the deaths occurred? Unfortunately, I could not find any historical data on deaths in aged care facilities in Australia. The Australian Bureau of Statistics (ABS) released a pilot study in 2021 on coding the location of death (eg at home, aged care, hospital etc) as a useful indicator. This covered data to 2019. But as I understand, this has not been implemented in their routine reporting.
On the other hand, there is detailed information on the number of COVID deaths in individual aged care facilities. In this government report there is a large list of possibly every aged care facility in the country and the number of COVID deaths for each. For the facility Kirsch identifies it says zero COVID deaths. There is a note saying:
Where a facility is reporting less than six resident or staff cases or less than six deaths, data has been suppressed to protect the privacy of affected individuals.
My understanding is that zero means zero in the data, for numbers less than 6 they say <6. However, on this Victorian state government page it indicates one COVID death for the facility. The Kirsch article confirms this. So, somehow the data did not get across to the federal agency. I note, from first-hand experience working on a project for a government department, collecting data from the states is usually a big mess, trying to aggregate data from different collection systems is a nightmare.
Cause Dementia
So what can we do? I decided to look at mortality caused by dementia as a possible surrogate for aged care. One can assume that a certain percentage of residents in aged care have dementia and so dementia deaths may be related to aged care deaths. I did the analysis and I found a result I wasn’t expecting.
The Dementia Australia website has some statistics on dementia.
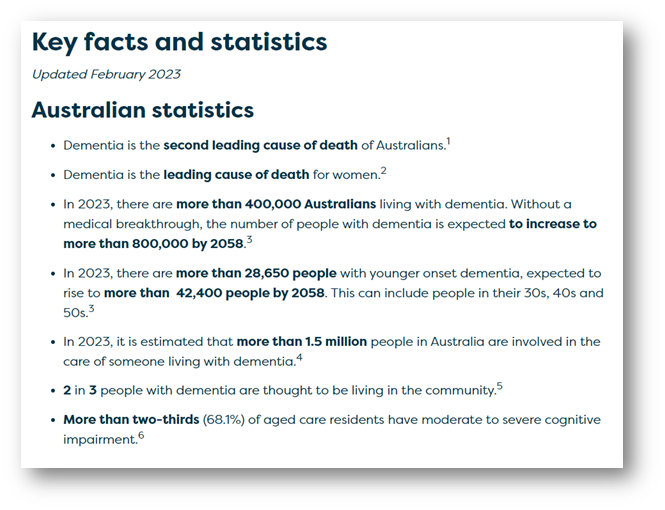
One third of all people with dementia reside in an aged care facility.
Two-thirds of aged care residents have some form of cognitive impairment.
And there are some other alarming statistics above about where it is heading.
The ABS provides mortality data by a number of causes of death. One of these is dementia, including Alzheimer’s disease. These are Doctor certified deaths (not including Coroner certified deaths). ABS Mortality reports are found on this page.
Up till March 2022 data was reported for individual weeks, on a monthly basis. Then it started being reported monthly. That made things a bit difficult to try to match weeks to months in graphs. I won’t bore with the details. Another complication is that when data is reported at a particular “provisional” release it always lags the actual data. This is because reports of death keep coming in. The numbers stabilise after about 2 months. So, we have to take this into consideration.
Here is a graph from the ABS of deaths due to dementia for years 2020 and 2021 with a baseline from 2015-2019 shown.

The orange 2020 line tracks above and below the baseline. The red line for 2021 is well above both the baseline and 2020.
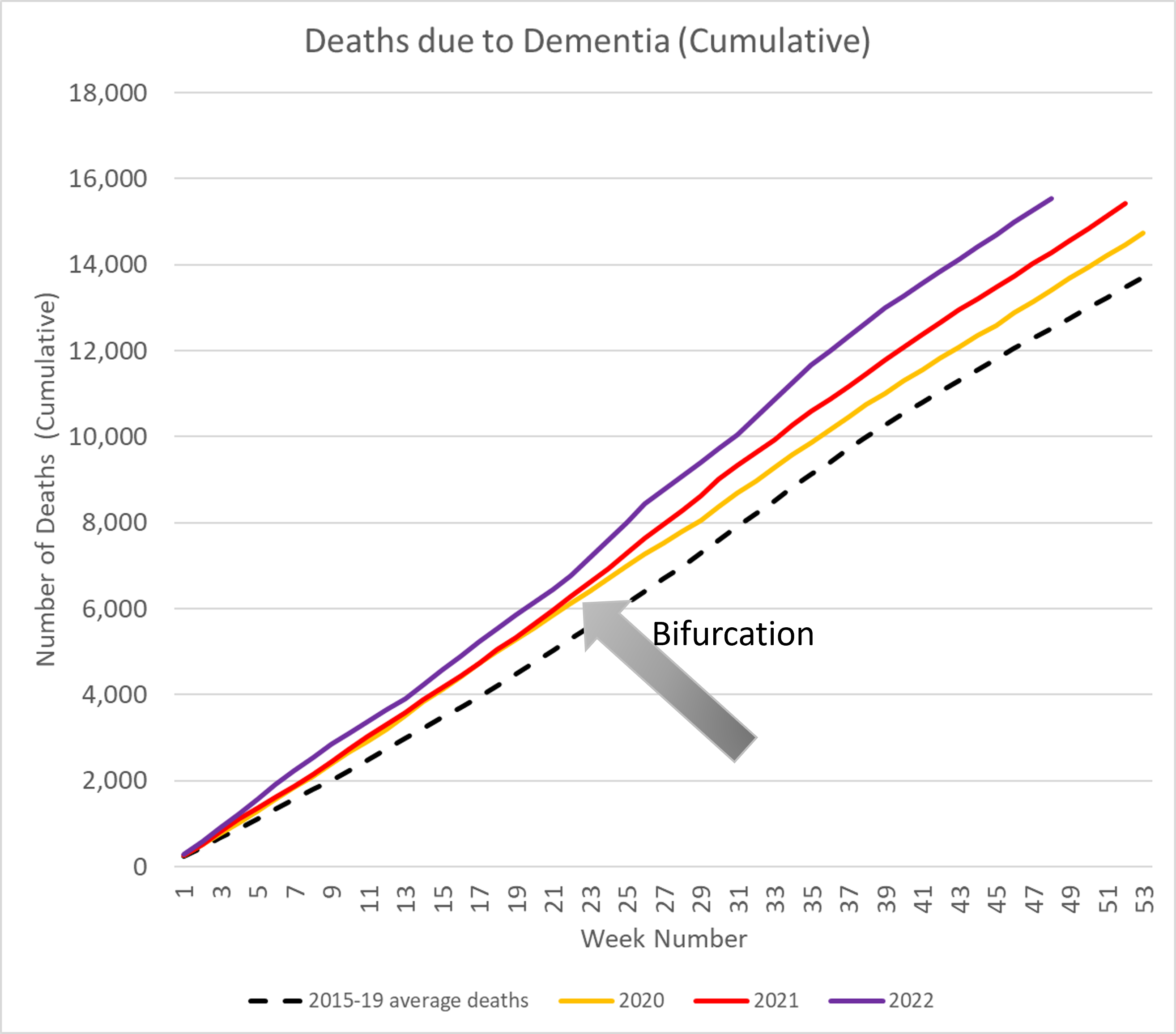
Now we have to take into consideration that with an aging population there is an increasing population of people with dementia. The ABS notes this. So, we expect mortality to increase year on year. Here’s my own graph of the weekly data available, including the start of 2022.

To handle the monthly data I decided to plot the cumulative number of deaths.

By interpolating the monthly data we can simultaneously show the data for 2022, which is currently available up till November.
Points to observe from this graph:
The value the lines reach at the right-hand side of the graph (end of the year) is the total number of deaths for a year. We see it progressively increasing across the years. The baseline is about 14,000 deaths in a year. For 2022 it is tracking to be over 16,000 deaths in a year.
The slope increasing, year on year, could be an indication of more people with dementia year to year and therefore more people dying. However, the increase we are seeing is greater than this.
COVID will have an effect. There is a lump at the beginning of 2022 (purple line) which will partly be due to COVID hitting Australia.
But the main point of interest is the bifurcation of the orange and yellow lines around week 23 (start of June). Any sudden changes are indicative of something different occurring.
In Australia the was no COVID at this time. From the worldometers site this graph charts COVID deaths in Australia.

The Delta wave started in September 2021. That’s around week 36. From November 2020 till then, there were no COVID deaths in Australia.
Let’s plot the difference between the successive years.

This is the result I wasn’t expecting. The jump is significant.
It is clear that the successive years were tracking the same, to within 100 deaths, until about the beginning of June 2021. From then, there are about 800 additional deaths in 2021, with the biggest jump occurring from June till the end of July.
Let’s look at what was happening in Australia around this time. Remember there was no COVID.
The vaccines were approved for use in January 2021 and started rolling out at the end of February 2021. In Australia there was some stuffing around and the rollout did not go as some thought it should, eg the experts, legacy media, government officials.
The Australian Prime Minister at the time, Scott Morrison was very averse to bad press. He was still reeling from the backlash of taking a holiday to Hawaii in the middle of the 2019-20 bush fires in NSW, the worst in our history (in terms of costliest natural disaster in Australia).

For overseas readers google terms Scott Morrison bushfires Hawaii and look at the images, you’ll get an idea of the backlash.
He had previously had success as Minister for Immigration in stopping people smugglers bringing illegal immigrants in via the north of Australia. He called the operation to turn back the boats Operation “Sovereign Border”. Politically this operation was a success but there was criticism of the harshness. So, to get the vaccine rollout going he decided another military operation was required. This time it was Operation “COVID Shield”.
An army General was appointed to be in charge. From the ABC news:

There was some criticism of this decision in defence circles that the military should not be dragged into what was a non-military problem.
Operation COVID Shield
The General got the vaccine rolling out. Operation COVID Shield started in June 2021. Aged care workers and residents were the first in line. A graph of the aged care rollout can be found here.

I indicate the official start date of the Operation. You can see that at the time the operation started things had slowed down, but in a matter of a month doses ramped up. Let’s go back to the dementia deaths in 2021 above 2020 and show when COVID Shield started.
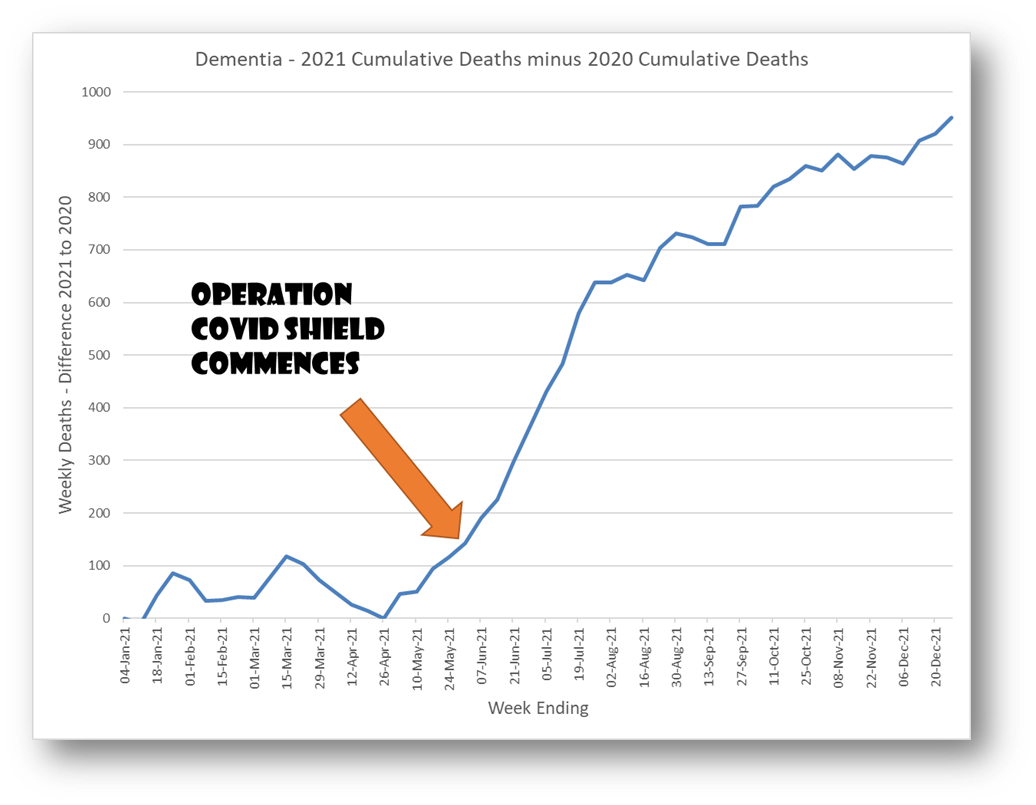
There was a rapid rollout to aged care. At the same time there was a large sudden increase in deaths of people with dementia.
There was no COVID. It was the start of Winter, but the Winter death peak, due to influenza, is usually in August in Australia.
The TGA Watches On
Very early on, even before the vaccines were available in Australia, data from Norway had indicated a number of deaths in elderly people from the Pfizer vaccine. Reported here.

From the article:
In a statement, Pfizer noted Norwegian authorities had prioritised the immunisation of residents in nursing homes, ‘most of whom are very elderly with underlying medical conditions and some of whom are terminally ill’…. The TGA also noted the deaths took place amongst a cohort including some expected to only have weeks or months to live, and moved to reassure the public that their approval process for vaccines is ‘extremely comprehensive and rigorous’.
This smacks of the TGA saying: well they were going to die anyway.
The deaths were associated with fever, nausea and diarrhoea – relatively common side effects after vaccination, which are very rarely dangerous in younger people.
So, is it OK to make these people suffer in their last days?
Under Freedom of Information this TGA correspondence was released. TGA’s Deputy Secretary Skerritt (soon to retire) knew in January 2021 about the data from Norway. But experts called for calm, as in the above article. More people were going to die from COVID.
And so the General marched on….
COVID Shield progressed and people with dementia sadly died.
Were these excess deaths, of people with dementia, caused by adverse reaction to injection? It may not even have been the physiological mechanisms of harm that have been identified from the mRNA technology. Just getting a terrible bout of diarrhoea could be the end. This are the people who can least care for themselves.
Another cause?
I was discussing the extra deaths in aged care with a colleague, a former barrister. He made a suggestion that there were government directives in place to defer sending people with illness in aged care facilities to hospitals. They had to be kept in the facilities. Presumably so the hospitals were not overrun.
In Australia, anyone who has had a loved one in an aged care facility knows how understaffed they are. There is a requirement for a registered nurse to be on duty but most of the staff are not medically trained. When someone is really sick they just don’t have the time to care for them. In pre-COVID years they got sent to the hospital for a stay until their health was at a level that the care in the aged care facility was sufficient.
Keeping people in aged care facilities when they should be sent to hospital will definitely lead to premature deaths.
The same thing happened in the UK. I saw this in a recent substack post from El Gato Malo covering the Hancock debacle.

This chart, that was obtained under FOI on hospital occupancy in the UK, shows the beds were empty in 2020.

Hospitals were nowhere near overrun.
We need to find the equivalent data for Australia. However, I suspect that this effect, of deferring sending people to hospital, has contributed to the gradual continuing increase in mortality over time. But may not explain the sudden rise we see from June to July in 2021 for people with dementia.
The politicians and bureaucrats in the UK were playing games with the population.

In Australia we shouldn’t expect any more competency than was demonstrated in the UK.
The Prime Minister thought a military solution was the answer to his problems. It was one size fits all. The TGA was too busy saying the approval process for vaccines is ‘extremely comprehensive and rigorous’.
I was trying to think of an analogy for a failed Shield. I use an example of a failure from the Space Shuttle program in a training course on analysis I run. The failure of the heat shield is an appropriate analogy. The shield is only good when all the tiles hold together. Once parts fall off disaster is waiting to happen. The mechanism of the failure is unexpected. Through providence failure doesn’t always occur. On two occasions it was disastrous.
The voice of experts, in their narrow fields, fueling mainstream media and terrifying the government of bad press coverage, is a recipe for disaster.
Another friend used an expression this week, while we were discussing another subject. It comes from a quote by an author H. L. Mencken. Paraphrased is goes:
"For every complex problem there is a solution that is clear, simple, and wrong."
Thanks for highlighting what's been happening to people with dementia. We care for my Mum, who has Alzheimer's at home. I looked back - we were in lock down at about that time. Aged care homes in Australia are a disgrace. People with dementia in residential care rely on loved ones to provide most of their care. This includes feeding, hydrating, managing incontinence and changing position to manage pressure areas. If you remember the Coroner's findings in the St Basil Nursing Home' deaths - residents died of malnutrition and dehydration (https://www.theguardian.com/australia-news/2022/jul/04/melbourne-aged-care-home-st-basils-charged-by-workplace-safety-watchdog-after-covid-deaths; https://www.abc.net.au/news/2021-11-22/st-basil-aged-care-home-melbourne-covid-coronial-hearing/100640490). Anecdotally I have also heard of residents that lost significant amounts of weight. Due to the vaccine mandates, there were also extreme staff shortages. The aged care workforce has quite a lot of discretionary workers. Those staff that did not want to get the vaccine or were not prepared to work under the conditions imposed in nursing homes left the sector. Hence, my hypothesis is that staff shortages and no loved ones to provide care, meant residents died (without any real oversight by the severely lacking Dept of Health) at a significantly faster rate than they otherwise would have. There are still significant staff shortages in aged care.
Having said that, I think you are also right to question the impact of the vaccine - we know that the spike protein impacts the epithelium - so, in particular the vasculature is inflamed. We know that the spike protein crosses the blood brain barrier - so increased inflammation in the brain. Have a look at the excellent work by Dale Bredesen on Alzheimer's - Alzheimer's is essentially brain inflammation. Get rid of the sources of brain inflammation (toxins, lack of neurotrophic support, insulin resistance, etc) reduce your risk of Alzheimer's or reverse Alzheimer's (https://www.apollohealthco.com/dr-bredesen/). I expect that the vaccine has increased the rate of deterioration of people with dementia in aged care.
Again, thanks for your attention to this sector of the community. Much more attention is needed.
Thank you for this. I was wondering when someone would connect the dots on the dementia aspect of the vaccines and lockdowns. Remember well two things: the lipid nanoparticles are designed to pass the blood-brain barrier (as per patents for oncolytic viruses - see the numerous patents by people at the University of Newcastle and Level 4 facility in Melbourne), and the Royal Commission into Aged care as below:
The Commissioners delivered an interim report on 31 October 2019, a special report on COVID-19 and aged care on 1 October 2020, and a final report on 26 February 2021. https://agedcare.royalcommission.gov.au/